The DPT vaccine or DTP vaccine is a class of combination vaccines against three infectious diseases in humans: diphtheria, pertussis (whooping cough), and tetanus. DTP vaccination was licensed in 1949. Since the introduction of the combination vaccine, there has been an extensive decline in the incidence of pertussis, or whooping cough, the disease which the vaccine protects against. Additionally, the rates of disease have continued to decline as more extensive immunization strategies have been implemented, including booster doses and increased emphasis on increasing health literacy [1].
Diphtheria is mostly caused by toxigenic Corynebacterium diphtheriae strains and occasionally by toxigenic C. ulcerans and C. pseudotuberculosis strains [1]. The acute respiratory infection caused by Diphtheria is generally characterized by local growth of the bacterium in the pharynx with pseudomembrane formation [2]. Then, Systemic dissemination of diphtheria toxin (DT) invokes lesions in distant organs. Diphtheria toxin is an exotoxin produced by the pathogen that inhibits protein synthesis and causes cell death [1, 2]. It is secreted across the cytoplasmic membrane without cell lysis. The mature extracellular toxin is a 58-kDa polypeptide comprising 535 amino acid residues. DT is endocytosed into the cells via the binding of its B-subunit to the proheparin-binding epidermal growth factor-like growth factor (HB-EGF) (Fig. 1); the ADP-ribosylation activity of DT prevents protein synthesis in the host cell and results in cell death [1].
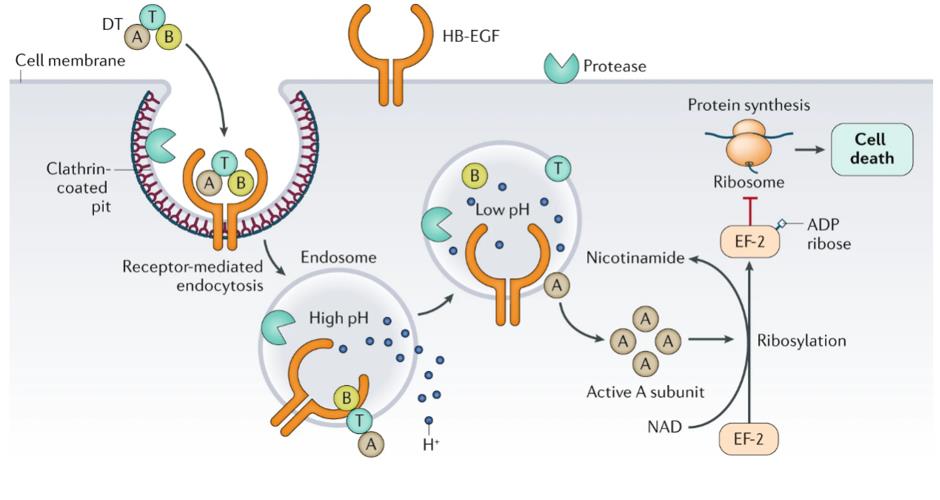 Fig. 1 Mechanism of action of DT
Fig. 1 Mechanism of action of DT
Pertussis, also known as whooping cough or the 100-day cough, is a highly contagious bacterial disease. The majority of human illness is caused by Bordetella pertussis, and some is caused by Bordetella parapertussis. B. pertussis contains 3,121 proteins, many of which are antigenic or biologically active. Fimbriae (FIM) are protein projections on the surface of B. pertussis which appear to function as adhesins. Filamentous hemagglutinin (FHA) is a component of the cell wall of all Bordetella spp. It is highly immunogenic and is the dominant attachment factor for Bordetella in animal model systems. Pertactin (PRN) is an outer membrane protein of B. pertussis that allows it to resist neutrophil-mediated clearance [3]. Some DTaP vaccines containing PRN in addition to pertussis toxin (PT) and FHA were shown to be more effective than those without. PT is a critical factor related to mortality in young infants and is unique to B. pertussis. PT is responsible for leukocytosis with lymphocytosis seen in B. pertussis infections in unimmunized individuals. Leukocytosis is a major risk factor for severe disease in unprotected infants [3].
Tetanus, also known as lockjaw, is a bacterial infection caused by Clostridium tetani, and is characterized by muscle spasms. Clostridium tetani produce the Tetanus neurotoxin (TeNT), which is released as a single polypeptide chain of 150 kDa. The long journey that TeNT undertakes to reach its neuronal targets within the CNS [4]. TeNT (red dots) enters peripheral nerve terminals within endosomes that undergo retroaxonal transport to the perikaryon. TeNT is then released in the external medium and binds to inhibitory interneurons impinging on the peripheral neurons as well as other inhibitory interneurons located at different levels of the spinal cord and of the brain stem: Once released from bacteria, TeNT enters the lymphatic and blood circulations [4, 5]. Consequently, it can be estimated that TeNT reaches the general circulation in a very short time, that is, minutes. Thereafter, TeNT undergoes retroaxonal transport inside motor and sensory neurons and it is released in the spinal cord where it blocks neurotransmitter release from inhibitory interneurons; this in turn impairs the balanced contraction of opposing skeletal muscles located in the anatomical area where TeNT was originally released (Fig. 2) [5]. It is important that the production and release of TeNT may continue for days leading eventually to a general distribution of TeNT in the body fluids with the consequent transition from a local to a generalized form of tetanus.
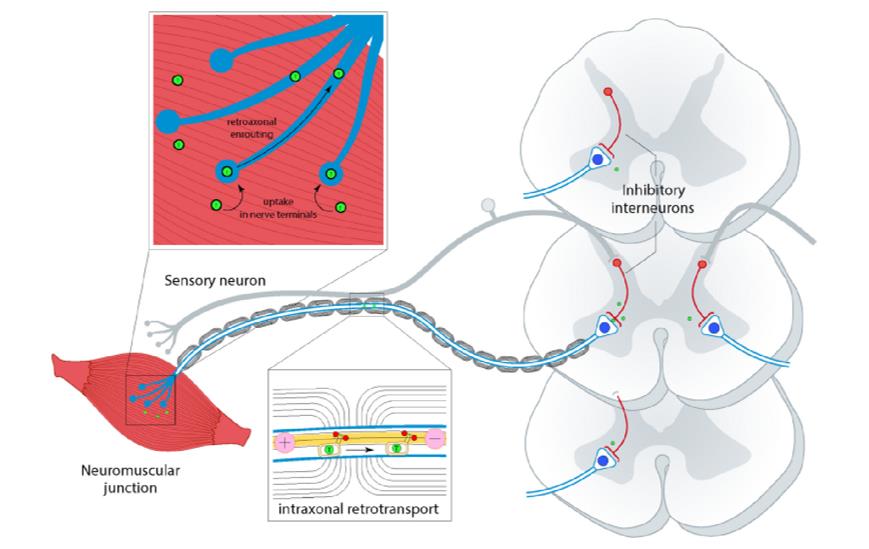 Fig. 2 The long journey that TeNT undertakes to reach its neuronal targets within the CNS. TeNT (red dots) enters peripheral nerve terminals within endosomes that undergo retroaxonal transport to the perikaryon. TeNT is then released in the external medium and binds to inhibitory interneurons impinging on the peripheral neurons as well as other inhibitory interneurons located at different levels of the spinal cord and of the brain stem.
Fig. 2 The long journey that TeNT undertakes to reach its neuronal targets within the CNS. TeNT (red dots) enters peripheral nerve terminals within endosomes that undergo retroaxonal transport to the perikaryon. TeNT is then released in the external medium and binds to inhibitory interneurons impinging on the peripheral neurons as well as other inhibitory interneurons located at different levels of the spinal cord and of the brain stem.
Starting in the US in 1948, DTP vaccines became the building block of childhood vaccines and were introduced in most industrialized countries. Following introduction, the number of notified cases and deaths declined significantly, accelerating the decline that was already being observed due to better medical treatment of infected infants. This success helped to prompt the WHO to embark on the 'Extended Programme of Immunization (EPI)' in 1977 in order to increase vaccine coverage with childhood vaccines such as DTP in all countries of the world [6]. The whole cell diphtheria-tetanus-pertussis vaccine (DTwP) has been replaced in many countries since the 1990s by corresponding acellular formulations (DTaP) due to their lower rates of severe adverse reactions [9]. In the decade between 1990 and 2000, vaccine producers developed, tested and licensed combination products such as DTaP-Hib vaccines (tetravalent), DTaP-Hib-polio vaccines (pentavalent), and finally DTaP-Hib-polio-HBV vaccines (hexavalent) [6].
DTaP (also DTPa and TDaP) is a combination vaccine against diphtheria, tetanus, and pertussis, in which the pertussis component is acellular. This is in contrast to whole-cell, inactivated DTP (DTwP). The acellular vaccine uses selected antigens of the pertussis pathogen to induce immunity. Because it uses fewer antigens than the whole-cell vaccines, it is considered to cause fewer side effects, but it is also more expensive [7].
VLP and NP vaccines are used in toxoid vaccine formulations in DTaP, which provide quick neutralization against a cytotoxic molecule (primarily bacterial toxins) that cannot be expressed in its full and activated form [8]. Review of the serologic data obtained from the efficacy studies demonstrated that the immunoglobulin G (IgG) PT levels detected by ELISA and the PT-neutralizing antibody responses to the responses seen with the DTaP (diphtheria toxoid, tetanus toxoid were significantly more than the DTwP vaccine, and acellular pertussis) vaccines included in the efficacy trials. Further more, the DTaP vaccines were associated with fewer adverse events than the DTwP vaccine, and most DTaP vaccines stimulated comparable or higher serum antibody responses than the DTwP vaccine [8-10].
DTaP vaccines induced both a type 1 and type 2 cytokine profile which induce a T-helper 17 (Th17) response, while the DTwP vaccine induced predominantly a type 1 pattern. It is indicated that the DTaP vaccines were better inducers of cell-mediated immune responses than the DTwP vaccine, particularly against PT, and the cell-mediated immune responses persisted, in contrast to the rapid decline in antibody levels. Generally, after a DTaP booster, higher memory B-cell responses and T-cell responses to antigens were demonstrated in acellular vaccine-primed children, compared with whole-cell vaccine-primed children. And that enhanced immunoglobulin E (IgE) and IgG4 responses to pertussis antigens are also noted after preschool booster vaccination at 4 years [11-12].
For better medical defense, A DTP vaccine that included a two-component acellular pertussis vaccine valence (containing Pertussis Toxoid [PT] and filamentous hemagglutinin [FHA] antigens) (i.e. DTaP) was developed. This DTaP vaccine is manufactured in France and constitutes the core of various combinations with other pediatric vaccine antigens, including a tetravalent DTaP-IPV vaccine, a pentavalent DTaP-IPV//PRP-T vaccine, and a hexavalent DTaP-IPV-HB-PRP~T vaccine, which have been studied extensively [13].
It has been shown that DTaP-IPV combined vaccine can produce the same or enhanced antibody response to several components of pertussis as DTP alone. There was no statistically significant difference between the antibody response to IPV and the response to IPV alone, without additional side effects [14]. Combining Hib with DTaP vaccine reduces the number of injections and visits to the clinic and increases vaccine coverage and compliance. The combination vaccine diphtheria and tetanus toxoids and acellular pertussis adsorbed, inactivated poliovirus and Haemophilus b conjugate (tetanus toxoid conjugate) vaccine (DTaP-IPV/Hib), which has been exclusively used in Canada for more than 10 years, is the first DTaP-based vaccine approved in the US that includes both poliovirus and Haemophilus influenzae type b (Hib) antigens [14, 15]. Administration of the DTaP-IPV/Hib vaccine as a four-dose series in infants provided high levels of seroprotection against diphtheria and tetanus toxoids, poliovirus types 1, 2, and 3, and Hib polyribosyl-ribitol-phosphate capsular polysaccharide conjugated to tetanus toxoid (PRP-T). Immune responses produced after doses 3 and 4 of DTaP-IPV/Hib vaccine were noninferior to those seen with separately administered DTaP, inactivated poliovirus, and Hib vaccines, apart from those against PRP-T in one study [13-16].
With several new vaccines for children awaiting licences (pneumococcal conjugate, meningococcal conjugate, hepatitis A, influenza) the need for combination vaccines will be increased. The advantages of combination vaccines, mainly the need for fewer injections and immunisation visits, should be balanced against the weaknesses, such as the perceived concerns about interaction and lower antibody titres. The advantages probably outweigh the concerns.
Emerging technologies and rational vaccine design, offer innovative approaches to address existing challenges of vaccine development. They have also significantly advanced our understanding of vaccine immunology and can guide future vaccine development for diseases [8]. Inactivated PT antigens can be directly produced by modification of PT genes using rDNA techniques (mutated twice to ensure no toxic reversal). The inactivated PT has stable long-term immunogenicity due to the absence of protein chemical denaturation. Increase the flexibility of production by increasing the promoter or copy number and using expression systems such as E. coli, yeast or insect cells to improve expression efficiency. Therefore, genetically engineered recombinant DTaP will be a direction for the development of combined vaccines. The technology will make the combined vaccine safer and more effective.
References