AIEC stands as a particular E. coli strain which shows strong connection to inflammatory bowel disease (IBD) through its association with Crohn's disease. AIEC differs from standard E. coli because it demonstrates targeted adherence to intestinal epithelial cells followed by cell invasion and intracellular survival and multiplication without immediate host cell death. The ability of AIEC to survive inside host cells enables it to avoid immune system detection while producing ongoing inflammation that leads to persistent intestinal inflammation. Research indicates AIEC exists more commonly in ileal tissue of Crohn's disease patients than in normal tissue samples which suggests its involvement in disease development.
The primary characteristic of AIEC bacteria is their strong ability to bind to intestinal epithelial cells. The bacterial adhesins on AIEC enable them to bind to host receptors which results in their ability to adhere to intestinal epithelial cells. The ileal epithelial cells of Crohn's disease patients express elevated levels of carcinoembryonic antigen-related cell adhesion molecule 6 (CEACAM6) which serves as a receptor for AIEC to establish selective colonization. The receptor-ligand connection between AIEC and CEACAM6 leads to better bacterial survival and extended mucosal colonization.
The bacteria establish contact with epithelial cells before they penetrate these cells through endocytic pathways. The invasion process of AIEC into epithelial cells occurs through endocytic pathways without causing major cell death to the host cells. The bacteria find a suitable environment inside host cell cytoplasm to multiply and create intracellular habitats.
AIEC bacteria demonstrate a unique ability to survive and multiply inside macrophages which makes them stand out from other bacteria. The normal process of phagocytosis leads bacteria to destruction by lysosomal enzymes. The bacteria manage to evade lysosomal destruction by multiplying inside the immune cells. The bacteria create a continuous inflammatory response in the intestinal mucosa through their ability to activate macrophages which produce pro-inflammatory cytokines.
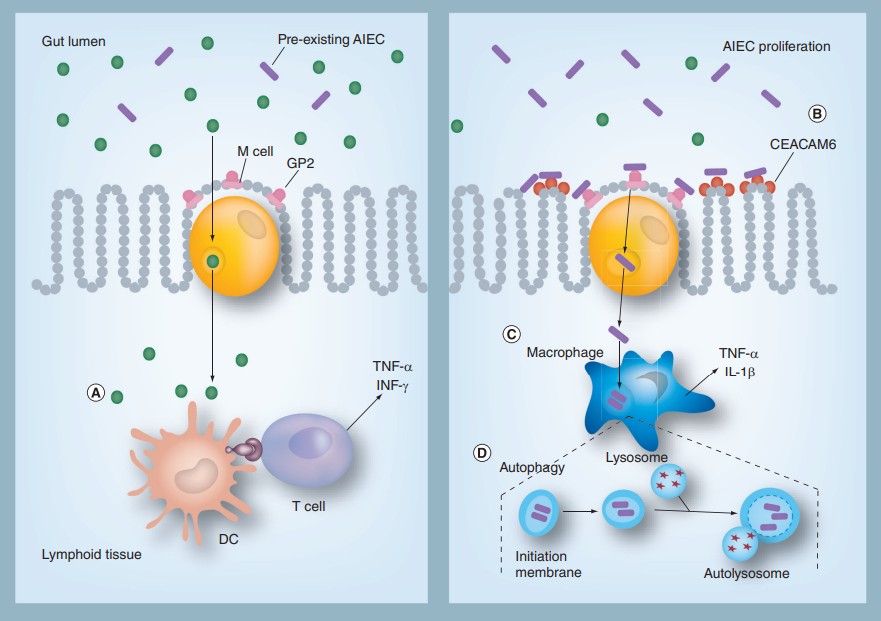 Figure 1. Model for adherent–invasive Escherichia coli pathogenesis. (Smith, 2013)
Figure 1. Model for adherent–invasive Escherichia coli pathogenesis. (Smith, 2013)
AIEC have been isolated in increased numbers from the guts of CD patients; however, they are also present in the guts of healthy individuals where they do not cause disease. Therefore AIEC can be considered to be pathobionts, that is, commensal organisms that can take advantage of a certain environment to cause disease. (A) AIEC may be present as normal members of the gut microbiota in humans. (B) Environmental insults, such as antibiotic therapy, induce a dysbiosis that selects for the proliferation of AIEC within the gut lumen. The resulting inflammatory response further contributes to the microbial dysbiosis in the gut and induces increased expression of CEACAM6, a receptor for AIEC on the surface of epithelial cells. (C) AIEC can invade epithelial cells and may also be taken up through the Peyer's patches via binding of long polar fimbriae (and type 1 fimbriae) to GP2 expressed on the surface of the M cells overlying the patches. (D) The AIEC are translocated to the macrophages (underlying the Peyer's patches or patrolling the lamina propria) where the bacteria can replicate within the phagosomes. The presence of AIEC results in the rapid induction of autophagy, killing the bacteria and resolving the infection. However, in some Crohn's disease patients, the presence of particular susceptibility alleles decreases the autophagy response and AIEC can therefore persist and replicate in their niche within the macrophages resulting in the hypersecretion of proinflammatory cytokines.
AIEC can also adhere to IECs through other host factors such as the Chitinase 3-like-1 (CHI3L1). CHI3L1, belonging to the glycohydrolase 18 family of chitinases, contains chitin-binding domain (CBD) and was reported to be upregulated during intestinal inflammation, predominately on IECs and lamina propria (LP) macrophages. Interestingly, an acute colitis can be exacerbated via CHI3L1 overexpression favoring bacterial adhesion and internalization into IECs. The bacterial chiA gene was identified in AIEC bacteria as involved in the interaction with IECs, and five conserved polymorphisms within the chiA gene were identified in pathogenic E. coli strains compared to nonpathogenic E. coli strains notifying that these polymorphisms may have been selected and could be associated to the virulence of AIEC bacteria.
 Figure 2. AIEC Mucosal Access and Colonization. (Chervy, 2020)
Figure 2. AIEC Mucosal Access and Colonization. (Chervy, 2020)
The detection of AIEC involves three main approaches which include functional phenotyping and molecular marker analysis and serological testing. The traditional cell-line phenotypic screening method using Caco-2, HT-29 and T84 cell lines assesses bacterial pathogenicity through adhesion and invasion and intracellular replication in macrophages and serves as the primary gold-standard assay. The development of PCR/qPCR assays for specific genes including fimH and pic and predictive models using 10-20 AIEC-specific SNPs has improved the speed of molecular identification for extensive strain collections. Clinically, measuring IgG antibodies against total E. coli in patient serum (AEcAb) with a defined cutoff provides a non‑invasive screening tool with a negative predictive value of 96.6 %; when combined with total E. coli counts in stool or biopsy specimens and an invasion threshold (>60 CFU per biopsy), the negative predictive value reaches 94.1 %. Additionally, MOS‑functionalized microgels that specifically bind the FimH adhesin can capture and remove AIEC ex‑vivo, offering both detection and "drug‑free" decontamination capabilities. Finally, high‑throughput genetic screens (e.g., type IV secretion system, gene knock‑outs) identify essential virulence genes, further refining molecular markers. By integrating these approaches, researchers can achieve precise identification and monitoring of AIEC across laboratory studies, clinical screening, and potential therapeutic strategies.
Pathogenic E. coli: Types, Toxins, and Detection Methods
Enteropathogenic E. coli (EPEC)
Enterotoxigenic E. coli (ETEC)
Enterohemorrhagic E. coli (EHEC)
Adherent invasive E. coli (AIEC)
Enteroaggregative E. coli (EAEC)
Diffusely-adhering E. coli (DAEC)
Verocytotoxigenic / Shiga toxin-producing E. coli (VTEC / STEC)
References
| Target | Cat. No. | Product Name | Host | |
| CHI3L1 | DAG-WT3348 | Native CHI3L1 Antigen | N/A | Inquiry |
| DAG-P0351 | Human CHI3L1 peptide | N/A | Inquiry | |
| DAG-P031 | Recombinant Human CHI3L1 Protein | HEK293 Cells | Inquiry |
| Target | Cat. No. | Product Name | Size | Species | Application | Detection Sample | |
| CEACAM6 | CKERS-CEACAM6-236H | Human Carcinoembryonic Antigen-related Cell Adhesion Molecule 6 (non-specific cross reacting antigen), CEACAM6 ELISA Kit | 5 plates | Human | Quantitative | Inquiry | |
| CEACAM6 | DEIA240 | Human CEACAM6/CD66c ELISA Kit | 96T | Human | Quantitative | Serum | Inquiry |
| CHI3L1 | DEIA-BJ2060 | Rat Cartilage glycoprotein 39/YKL40 ELISA Kit | 96T | Quantitative | Serum, plasma, cell culture supernatants, body fluid and tissue homogenate | Inquiry | |
| CHI3L1 | DEIA2905 | Mouse Chitinase 3-like 1 ELISA Kit | 96T | Mouse | Quantitative | cell culture supernatants, serum, plasma | Inquiry |
| CHI3L1 | DEIA7855 | Human CHI3L1(Chitinase-3-like protein 1) ELISA Kit | 96T | Human | Quantitative | Serum, plasma, tissue homogenates and other biological fluids | Inquiry |
| CHI3L1 | DIA-XYA138 | Chitinase 3-Like 1 ELISA Kit | 96T | Quantitative | cell lysates, serum, plasma | Inquiry |