Mouse Anti-Testosterone monoclonal antibody for ELISA
| Product Name | Cat. No. | Applications | Host Species | Datasheet | Price | Add to Basket |
|---|
| Product Name | Cat. No. | Applications | Host Species | Datasheet | Price | Add to Basket |
|---|
Testosterone (T) is an androgen produced by the testes that is crucial for maintaining spermatogenesis and sperm quality. Testosterone helps the growth of bones, muscles, and the testes, penis, and prostate, making male development, fertility, and health throughout life dependent on testosterone. Although the levels of testosterone in females are lower, research indicates that an appropriate amount of testosterone is beneficial for women's sexual function, bone health, and overall well-being. Approximately 95% of circulating testosterone is synthesized by the testes, with Leydig cells in the interstitial tissue of the testes producing testosterone in response to luteinizing hormone (LH) stimulation. LH is a glycoprotein hormone secreted by the pituitary gland, released in response to the pulsatile secretion of gonadotropin-releasing hormone (GnRH) from the hypothalamus. The total amount of testosterone in the blood, including free testosterone and protein-bound testosterone, is referred to as the circulating total testosterone level. Free testosterone accounts for about 2-3% of the total testosterone and can freely enter cells and exert biological effects; bound testosterone accounts for about 97-98% of the total testosterone, with most of it bound to sex hormone-binding globulin (SHBG) and a small portion bound to albumin. Only free testosterone and albumin-bound testosterone can be utilized by tissues.
Damage to interstitial cells, decreased pituitary LH drive or a combination of the two, together with high SHBG levels might impair testosterone bioavailability, resulting in testosterone deficit (TD). Low testosterone levels can inhibit spermatogenesis from advancing past the meiosis stage, leading to decreased sexual function and even infertility. It can also cause osteoporosis and cardiovascular disease, reducing muscle strength and coordination, as well as mental health issues like anxiety, sleep disturbances and cognitive impairment. Traditionally, testosterone replacement treatment (TRT) has been used to treat TD, however the exogenous injection of testosterone frequently causes immunological reactions that produce anti-testicular antibodies, which hinder spermatogenesis. Stimulating Leydig cells to make testosterone rather than delivering testosterone exogenously can raise serum testosterone levels while having no deleterious influence on spermatogenesis.
Reduced testosterone is also linked to obesity and type II diabetes. Obesity is thought to be the leading cause of TD in developed countries, with more than half of obese men suffering from the disease. Testosterone regulates the release of pro-inflammatory cytokines, which has an effect on fat levels. Testosterone activates androgen receptors (AR) and estrogen receptors (ER) α and β, reducing the release of adipokines such as leptin, IL-6, and TNF-α, increasing the production of adiponectin, and reducing the incidence of chronic diseases like type II diabetes. It also increases insulin activity, inhibits fat cell metabolism, and reflects anti-inflammatory activity.
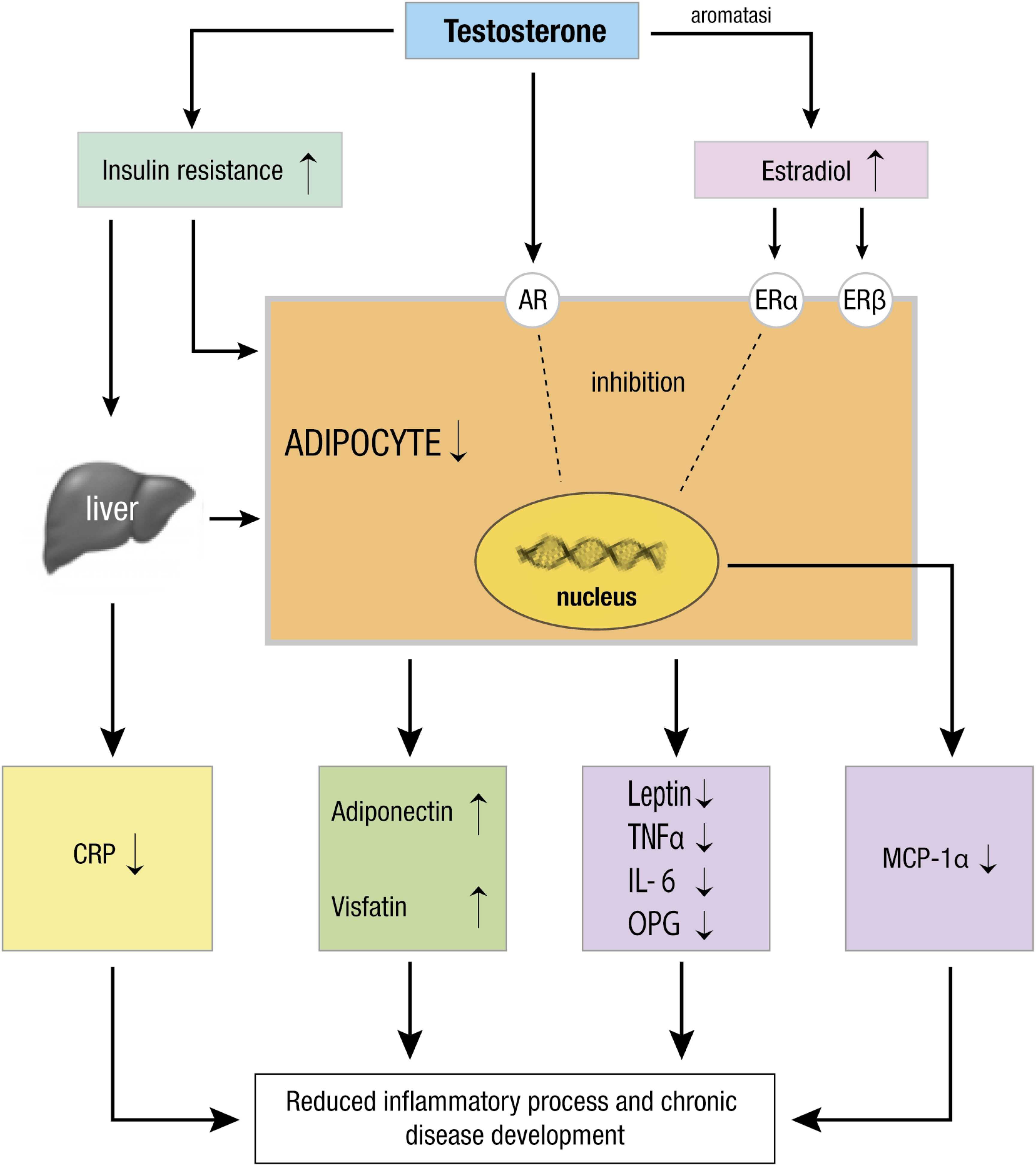 Figure 1. Testosterone exerts its anti-inflammatory activity through different mechanisms (Source: Bianchi VE, 2019)
Figure 1. Testosterone exerts its anti-inflammatory activity through different mechanisms (Source: Bianchi VE, 2019)
Testosterone Monoclonal Antibody, Clone 4H9B5
Mouse Anti-Testosterone Monoclonal Antibody, Clone 4H9B5
Monoclonal Antibody to Testosterone, Clone CHO/4H9B5
4H9B5 Anti-Testosterone Monoclonal Antibody
References
1. Bianchi VE. The anti-inflammatory effects of testosterone. J Endocr Soc. 2019;3(1):91-107.
![]()

