Crohn's disease (CD) and ulcerative colitis (UC) are the two main types of the chronic illness known as inflammatory bowel disease (IBD). Biologics have completely changed the way IBD is treated in recent years, improving patient results and quality of life. The immunogenicity of anti-drug antibodies (ADA) is a significant barrier, nevertheless. ADAs are produced by the immune system in reaction to biologics, such as recombinant protein medications and monoclonal antibodies. These antibodies thus decrease the efficiency of medications and cause negative side effects that jeopardize patient safety.
Th17 cells are considered as the primary pathogenic element driving disease progression. IBD patient intestinal mucosa shows extensive infiltration of Th17 cells together with notable increases in IL-17 and several pro-inflammatory cytokines. Activated transcription factor STAT3 leads to Th17 differentiation but Th17 generation stops when STAT3 is deficient.
The gut microbiota serves as a critical factor in IBD development. Variations in intestinal microbiota composition can lead to excessive Th17 cell growth which compromises the intestinal barrier function and causes IBD-associated inflammation. Despite IL-17A's role as a pro-inflammatory cytokine it becomes clear through certain IBD models that blocking IL-17A can worsen inflammation which implies IL-17A serves a protective function in certain conditions.
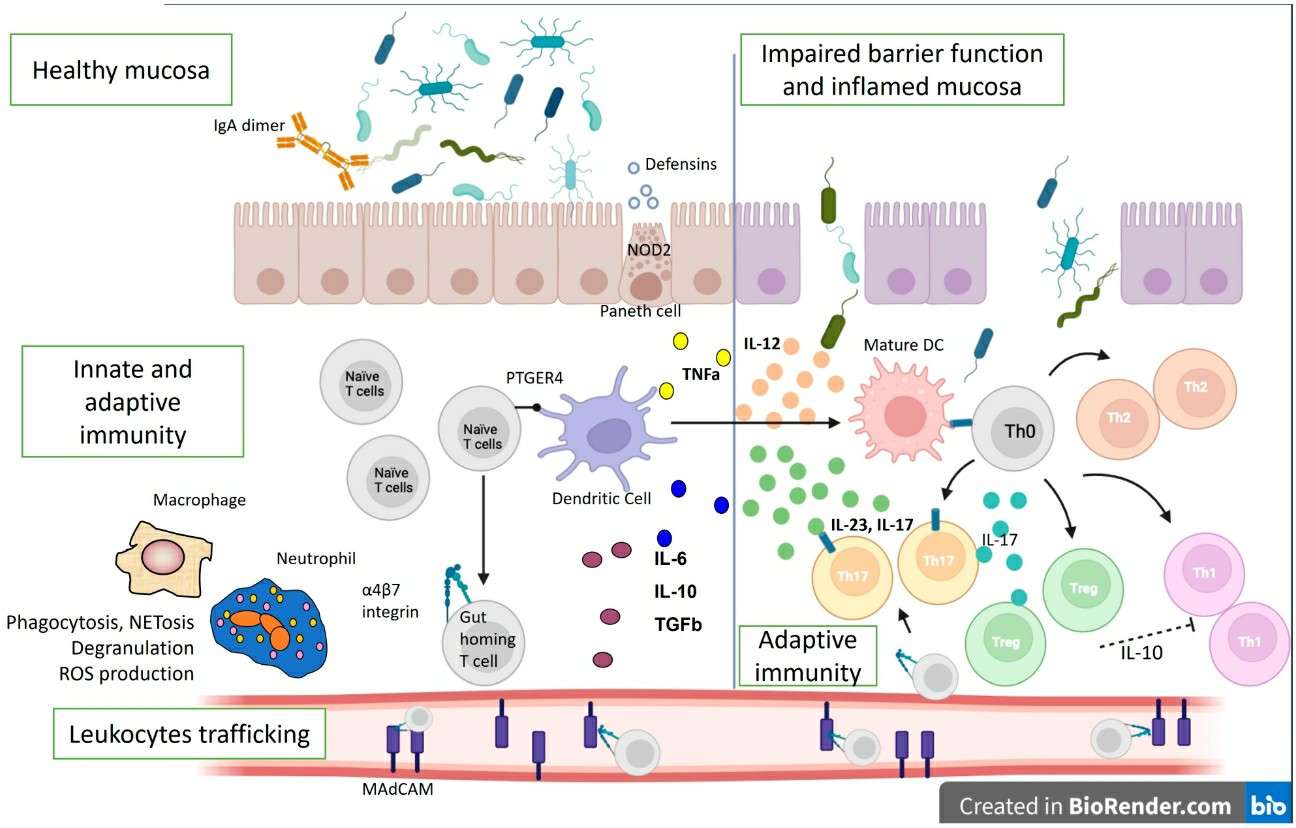 Figure 1. Immune Mechanisms in the Pathogenesis of IBD (Source: Velikova T, et al. 2024)
Figure 1. Immune Mechanisms in the Pathogenesis of IBD (Source: Velikova T, et al. 2024)
The main treatment strategies for IBD consist of small-molecule anti-inflammatory drugs such as 5-ASA and corticosteroids together with large-molecule biologic therapies. Biologics mainly include:
Among them, TNF monoclonal antibodies constitute essential biologic therapies for IBD. Adalimumab functions as a fully humanized monoclonal antibody against TNF-α which provides outstanding results for remission induction and maintenance in moderate-to-severe active Crohn's disease and ulcerative colitis leading to its widespread use for these conditions. Although biologics are fundamental to treatment protocols some patients may not respond initially or later lose their response to treatment.
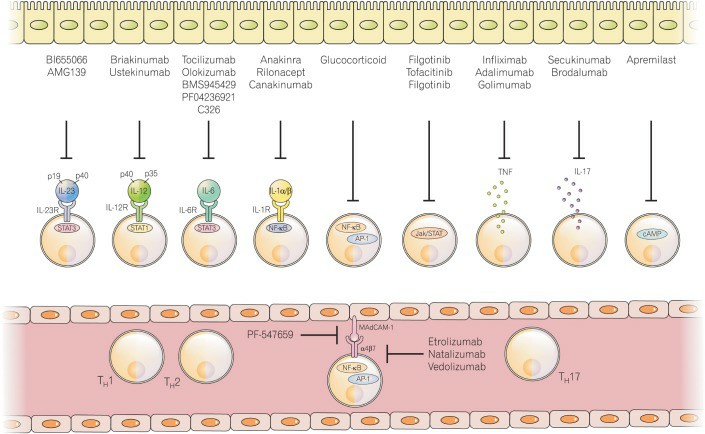 Figure 2. IBD Treatment Strategies Involving the Prevention or Inhibition of T Cell and Innate Lymphoid Cell (ILC) Generation (Source: Lee SH, et al. 2018)
Figure 2. IBD Treatment Strategies Involving the Prevention or Inhibition of T Cell and Innate Lymphoid Cell (ILC) Generation (Source: Lee SH, et al. 2018)
Biologics have greatly enhanced treatment results for IBD patients but treatment failure remains for some individuals. Secondary loss of response stands as a major reason along with individual genetic differences and gut microbiota influences as well as primary non-response. Extended biologic therapy can speed up drug elimination and create drug resistance while certain patients experience anti-drug antibody development after receiving anti-TNF-α treatment.
The development of ADAs represents a prevalent immunogenicity problem in every type of biologic therapy. Anti-TNF-α antibodies and similar biologics may trigger an immune response because the body identifies them as foreign entities which leads the immune system to create specific ADAs. The produced ADAs attach directly to the medication to create antigen-antibody complexes.
The development of ADAs plays a vital role in determining the effectiveness of IBD treatment and shaping patient outcomes.
The development of ADAs depends on several factors such as drug dosage levels, how often the drug is given, patients' immune system conditions and the use of immunomodulators alongside treatment. The rate at which anti-drug antibodies develop among IBD patients typically falls between 10% and 30%.
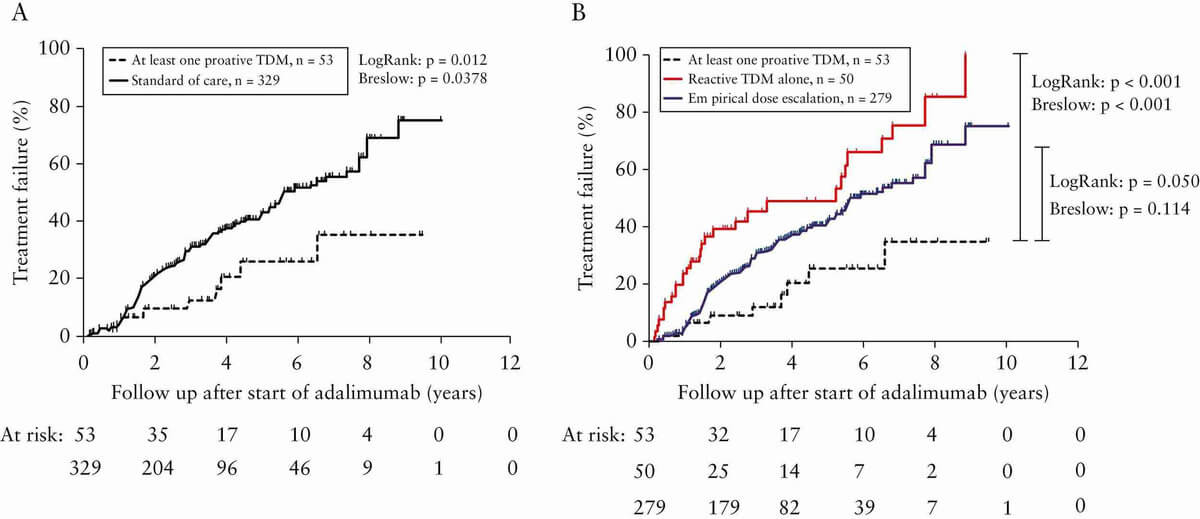 Figure 3. Example: Kaplan-Meier Cumulative Probability Curve of Treatment Failure in IBD Patients (Source: Papamichael K, et al. 2019)
Figure 3. Example: Kaplan-Meier Cumulative Probability Curve of Treatment Failure in IBD Patients (Source: Papamichael K, et al. 2019)
Clinical practice now employs multiple strategies to minimize ADA formation and enhance treatment results. Clinical research demonstrates that using immunomodulators such as azathioprine and methotrexate together results in significant reductions in ADA formation rates. When used together with adalimumab, azathioprine treatment leads to a substantial decrease in ADA formation rates and better treatment outcomes.
Therapeutic drug monitoring (TDM) serves as a fundamental tool in ADAs management. Boosting drug dosage can regain therapeutic effectiveness when both drug concentrations and ADA levels are deficient. Patients who have high levels of ADA may not benefit from dose modifications. Both drug levels and ADA measurements need to be checked prior to making any dosage changes. The introduction of an immunomodulator can effectively manage patients who exhibit the presence of ADAs.
The development of biosimilars has recently expanded treatment possibilities for IBD. Simlandi represents a high-concentration biosimilar of adalimumab which may offer benefits through reduced immunogenicity while being interchangeable.
While large-molecule biologics represent a major advancement in IBD therapy, a subset of patients still face treatment failures or drug resistance. Anti-drug antibodies present significant challenges that must be addressed during IBD treatment. Researching immunogenicity mechanisms further will lead to the development of superior treatment and prevention strategies that will provide improved results for IBD patients.
References
| Target | Cat. No. | Product Name | Size | Species | Application | Detection Sample | |
| Exendin-4 | DEIABL206 | Exendin-4 ADA ELISA kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| TNF | DEIA068J | TNF α-Blocker ADA, Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | serum, EDTA plasma | Inquiry |
| DEIA069J | TNF α-Blocker ADA, Total Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | serum, EDTA plasma | Inquiry | |
| DEIA018J | TNF α-Blocker ADA, Antibodies against etanercept ELISA Kit | 96T | Human | Qualitative | EDTA plasma, serum | Inquiry | |
| DEIA019J | TNF α-Blocker ADA, Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | EDTA plasma, serum | Inquiry | |
| DEIA020J | TNF α-Blocker ADA, Total Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | EDTA plasma, serum | Inquiry |
| Target | Cat. No. | Product Name | Size | Species | Application | Detection Sample | |
| Semaglutide | DEIASL092 | Semaglutide ELISA Kit | 96T | NA | Quantitative | Serum, plasma | Inquiry |
| Ramucirumab | DEIAZ0009 | Anti-Ramucirumab ELISA Kit | 96T | Human | Qualitative | Serum, plasma | Inquiry |
| Filgrastim | DEIABL228 | Filgrastim Elisa kit | 2 x 96T | Human | Quantitative | Serum, plasma | Inquiry |
| Liraglutide | DEIA-XYZ95 | Liraglutide High Sensitivity Elisa Kit | 96T | NA | Quantitative | Serum, plasma | Inquiry |
| MMAE | DEIABL314 | Intact MMAE ADC ELISA Kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| DM1 | DEIABL311 | DM1 ADC ELISA Kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| SN38 | DEIABL316 | SN38 ADC ELISA Kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| Eculizumab | DEIAZ0063 | Eculizumab ELISA kit | 96T | NA | Quantitative | Serum, plasma, cell culture samples | Inquiry |