Pharmacokinetics (PK) investigates how drugs interact with the human body throughout their exposure period following administration. The main goal involves mapping out how a drug travels through the body and the mechanisms for its removal. This process mainly involves four steps: In pharmacokinetics four key phases work together which include absorption, distribution, metabolism, and excretion and professionals use the acronym ADME to describe them.
Multiple factors influence drug metabolism including age where seniors have a slower processing rate increasing toxicity risk and infants need dose adjustments due to immature liver functionality together with drug interactions that modify enzyme activity and genetic variations like CYP2D6 gene variants that impact drug effectiveness and safety.
 Figure 1. Multiple Clearance Pathways Affecting the Pharmacokinetics of a mAb (Source: Ryman JT, Meibohm B. et al. 2017)
Figure 1. Multiple Clearance Pathways Affecting the Pharmacokinetics of a mAb (Source: Ryman JT, Meibohm B. et al. 2017)
Apart from the ADME definition, several key parameters in PK research should be understood:
Cmax (maximum plasma concentration): The highest concentration of the drug in the blood.
Tmax (time to peak concentration): The time it takes to reach the maximum plasma concentration.
AUC (area under the curve): The total exposure to the drug in the body.
t½ (half-life): The time required for the drug concentration to decrease by half.
CL (clearance): The body's ability to eliminate the drug.
Vd (volume of distribution): A measure of how the drug is distributed in the body's tissues.
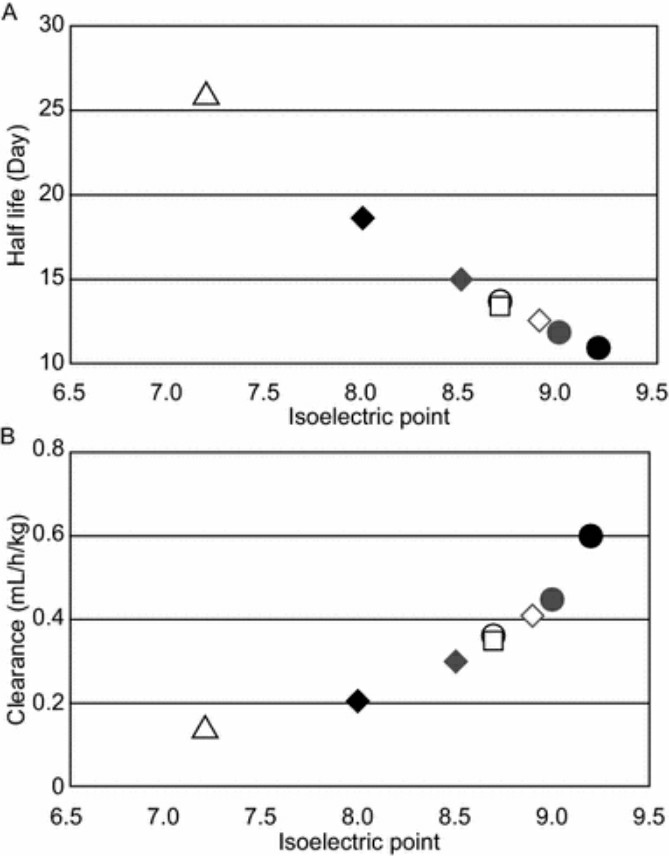 Figure 2. Relationship Between Charge/pI and Half-life and Clearance in PK of mAbs (Source: Igawa T, et al. 2018)
Figure 2. Relationship Between Charge/pI and Half-life and Clearance in PK of mAbs (Source: Igawa T, et al. 2018)
PK assessments of macromolecular drugs such as monoclonal antibodies and peptide medicines show more complexity and significance than those of small molecules. The processes of absorption and elimination in macromolecular drugs differ from those of small molecules. Macromolecular drugs are delivered to the body via subcutaneous or intravenous injection and their distribution relies on target binding plus recycling through FcRn mechanisms. Macromolecular drugs undergo metabolism through protein degradation pathways rather than enzymatic processes and are cleared via protein degradation and receptor-mediated endocytosis as well as cellular phagocytosis instead of liver enzymes or kidney excretion.
PK testing for macromolecular drugs faces several challenges:
The intricate requirements for sample preparation and separation processes prevent macromolecular drugs from being adequately tested with standard LC-MS/MS methods which are designed for small molecules. ECL and CLIA require expensive equipment and reagents and operate under strict experimental conditions which decrease accessibility and create higher usage challenges. The ELISA technique leads macromolecular drug testing methods with unmatched specificity and sensitivity. Pharmacists measure the concentration of monoclonal antibodies including adalimumab and trastuzumab in blood samples using ELISA to establish optimal dosages. ELISA enables the analysis of DM1 ADC and SN38 ADC antibody-drug conjugates through simultaneous measurement of both unbound antibodies and drug conjugation levels.
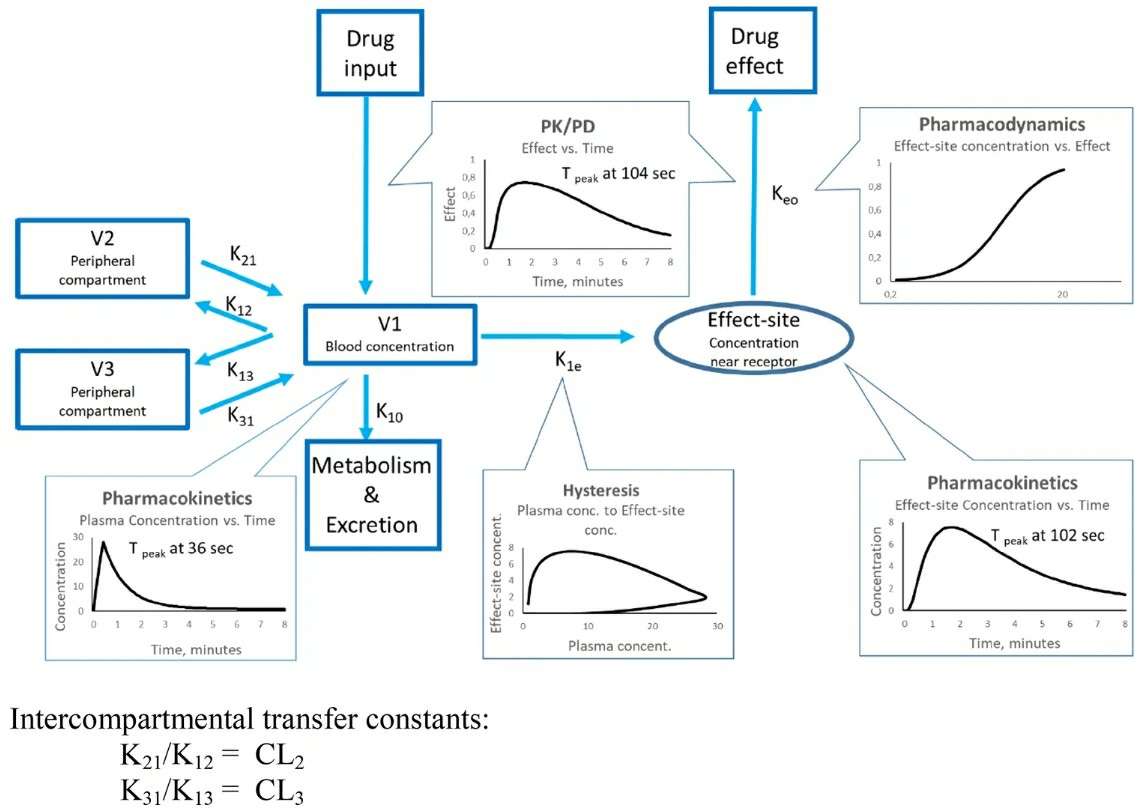 Figure 3. Overview of a Three-Compartment Pharmacokinetic/Pharmacodynamic Model (Source: Sahinovic M, Struys MM, Absalom AR. et al. 2018)
Figure 3. Overview of a Three-Compartment Pharmacokinetic/Pharmacodynamic Model (Source: Sahinovic M, Struys MM, Absalom AR. et al. 2018)
ELISA quantifies drug concentrations and identifies ADA to monitor biological immune response to biologics. ELISA data provides guidance for personalized treatments and supports tailored therapy development when it is integrated with PK/PD modeling. Creative Diagnostics offers advanced PK analysis kits which we believe will optimize your work with biologic drugs. Get in touch with us to get more information about macromolecular drugs and PK & ADA analysis while learning how we can support you!
References
| Target | Cat. No. | Product Name | Size | Species | Application | Detection Sample | |
| Exendin-4 | DEIABL206 | Exendin-4 ADA ELISA kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| TNF | DEIA068J | TNF α-Blocker ADA, Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | serum, EDTA plasma | Inquiry |
| DEIA069J | TNF α-Blocker ADA, Total Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | serum, EDTA plasma | Inquiry | |
| DEIA018J | TNF α-Blocker ADA, Antibodies against etanercept ELISA Kit | 96T | Human | Qualitative | EDTA plasma, serum | Inquiry | |
| DEIA019J | TNF α-Blocker ADA, Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | EDTA plasma, serum | Inquiry | |
| DEIA020J | TNF α-Blocker ADA, Total Antibodies against infliximab ELISA Kit | 96T | Human | Qualitative | EDTA plasma, serum | Inquiry |
| Target | Cat. No. | Product Name | Size | Species | Application | Detection Sample | |
| Semaglutide | DEIASL092 | Semaglutide ELISA Kit | 96T | NA | Quantitative | Serum, plasma | Inquiry |
| Ramucirumab | DEIAZ0009 | Anti-Ramucirumab ELISA Kit | 96T | Human | Qualitative | Serum, plasma | Inquiry |
| Filgrastim | DEIABL228 | Filgrastim Elisa kit | 2 x 96T | Human | Quantitative | Serum, plasma | Inquiry |
| Liraglutide | DEIA-XYZ95 | Liraglutide High Sensitivity Elisa Kit | 96T | NA | Quantitative | Serum, plasma | Inquiry |
| MMAE | DEIABL314 | Intact MMAE ADC ELISA Kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| DM1 | DEIABL311 | DM1 ADC ELISA Kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| SN38 | DEIABL316 | SN38 ADC ELISA Kit | 96T | Human | Quantitative | Serum, plasma | Inquiry |
| Eculizumab | DEIAZ0063 | Eculizumab ELISA kit | 96T | NA | Quantitative | Serum, plasma, cell culture samples | Inquiry |