Endometrial cancer is a group of epithelial malignant tumors that occur in the endometrium and are more common in perimenopausal and postmenopausal women. Endometrial cancer is one of the most common tumors of the female reproductive system, with nearly 200000 new cases each year, and is the third most common gynecological malignancy causing death (after ovarian cancer and cervical cancer). Its incidence is closely related to lifestyle, and its incidence rate varies from region to region. In North America and Europe, its incidence is only second to breast cancer, lung cancer, colorectal cancer, and ranks first in female reproductive system cancer. In China, with the development of society and the improvement of economic conditions, the incidence rate of endometrial cancer has also increased year by year, second only to cervical cancer, ranking second in malignant tumors of the female reproductive system.
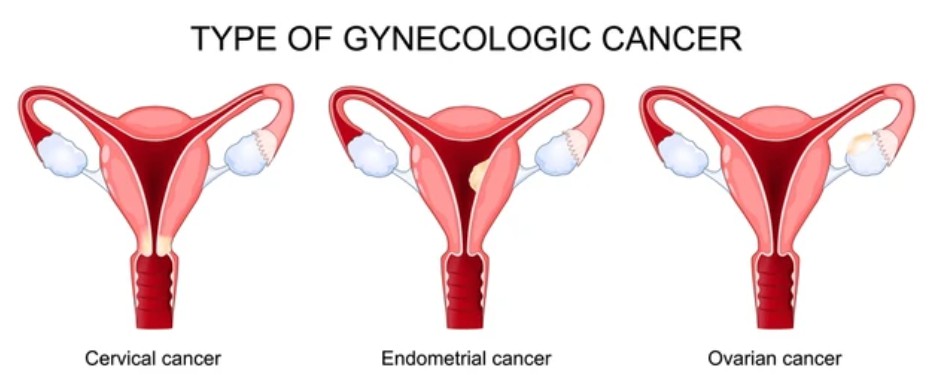 Figure 1. Endometrial Cancer.
Figure 1. Endometrial Cancer.
| Symptoms | Descriptions |
|---|---|
| Bleeding | Irregular vaginal bleeding is the main symptom of endometrial cancer, often consisting of small to moderate amounts of bleeding. Young women or perimenopausal women often mistake it for menstrual irregularities and overlook it. Postmenopausal women often present with persistent or intermittent vaginal bleeding. Some patients only present with a small amount of bloody vaginal discharge after menopause. Late-stage patients may have minced meat-like tissue mixed in during bleeding. |
| Vaginal discharge | Patients with vaginal discharge may experience varying degrees of vaginal discharge. In the early stages, it may present as thin white discharge or a small amount of bloody vaginal discharge. If combined with infection or cancer necrosis, there may be purulent discharge accompanied by odor. Sometimes vaginal discharge may be accompanied by tissue-like substances. |
| Pain | Cancer lesions and the resulting bleeding or infection can stimulate uterine contractions, causing paroxysmal lower abdominal pain. Postmenopausal women may experience severe lower abdominal pain and fever due to poor drainage of uterine secretions caused by cervical canal stenosis, which can lead to secondary infection and accumulation of pus in the uterine cavity. When cancer tissue infiltrates and penetrates the entire layer of the uterus in the late stage of the tumor, or invades the connective tissue, cervical ligaments, bladder, intestinal tract, or infiltrates and compresses the pelvic wall tissue or nerves, it can cause persistent and gradually worsening pain, accompanied by lumbosacral pain or radiating to the same lower limb. |
| Abdominal lump | Early endometrial cancer generally cannot reach the abdominal mass. If endometrial cancer is combined with larger uterine fibroids, or if there is late-stage accumulation of pus in the uterine cavity and metastasis to the pelvic and abdominal cavity to form a huge mass (such as ovarian metastasis), the mass may be palpable in the abdomen, generally solid, with poor mobility and sometimes tenderness. |
| Symptoms | Descriptions |
|---|---|
| B-ultrasound examination | B-ultrasound examination can determine the size of the uterus, thickness of the endometrium, presence of uneven echoes or intrauterine growths, presence and degree of muscle infiltration, etc. Its diagnostic accuracy rate is over 80%. Due to the high number of obese patients with endometrial cancer, transvaginal ultrasound has more advantages than transabdominal ultrasound. Due to its convenience and non-invasiveness, B-ultrasound has become the most routine examination for diagnosing endometrial cancer and a preliminary screening method. |
| Segmented diagnosis and scraping | It is the most commonly used and valuable method for diagnosing endometrial cancer. Not only can it clarify whether it is cancer and whether endometrial cancer involves the cervical canal, but it can also differentiate between endometrial cancer and cervical adenocarcinoma, thereby guiding clinical treatment. For patients with significant vaginal bleeding or continuous bleeding during perimenopause, staged curettage can also help to stop bleeding. The specimens for segmented scraping need to be labeled separately and sent for pathological examination in order to confirm or exclude endometrial cancer. |
| Hysteroscopy examination | Under hysteroscopy, the presence, location, size, and extent of cancer lesions in the uterine cavity and cervical canal can be directly observed, as well as whether the cervical canal is affected; Direct visualization for biopsy of suspicious lesions can help detect smaller or earlier lesions and reduce the missed diagnosis rate of endometrial cancer. The accuracy of biopsy under hysteroscopy is close to 100%. Hysteroscopy and segmental curettage can cause complications such as bleeding, infection, uterine perforation, cervical laceration, and comprehensive reactions to abortion. Hysteroscopy also carries the risk of water poisoning. There is still controversy over whether hysteroscopy can lead to the spread of endometrial cancer. Currently, most studies believe that hysteroscopy does not affect the prognosis of endometrial cancer. |
| Magnetic resonance imaging (MRI) | MRI can clearly display the size and extent of endometrial cancer lesions, muscle infiltration, and pelvic and para aortic lymph node metastasis, thereby accurately estimating tumor staging. CT has slightly lower resolution for soft tissue than MRI, so in hospitals with the necessary conditions, there are more patients who use MRI for preoperative evaluation. |
The treatment principles for endometrial cancer should be based on the patient's age, physical condition, lesion scope, and histological type, and appropriate treatment methods should be selected. Due to the fact that the vast majority of endometrial cancer is adenocarcinoma and is not very sensitive to radiation therapy, surgery is the main treatment, with other comprehensive treatments such as radiotherapy and chemotherapy. Early patients are mainly treated with surgery, and adjuvant therapy is selected based on the results of surgical pathological staging and high-risk factors for recurrence; Late stage patients are treated with a combination of surgery, radiotherapy, and chemotherapy.
Surgery: Surgery is the primary treatment for endometrial cancer. For early patients, the surgical objective is to stage the disease through surgery pathology, accurately determine the extent of the lesion and its prognosis, remove the affected uterus and potential metastatic lesions, and determine the choice of postoperative adjuvant therapy. The surgical procedures generally include abdominal flushing fluid examination, extrafascial total hysterectomy, bilateral oophorectomy and salpingectomy, pelvic lymph node dissection+/- para aortic lymph node dissection.
Radiotherapy: Simple radiotherapy is only suitable for elderly and weak patients, those with severe internal medicine complications who cannot tolerate surgery or are contraindicated for surgery, and those who are not suitable for surgery in stage III or above, including intracavitary and extracorporeal irradiation. Preoperative radiotherapy is rarely used, but for patients with severe vaginal bleeding, poor condition, multiple complications, and short-term intolerance to surgery, radiotherapy can be used first to stop bleeding and control disease progression.
Endometrial cancer is an important health issue of concern for women worldwide, closely related to hormonal imbalances and lifestyle factors. Early detection and appropriate treatment are crucial for improving prognosis and survival rates. The progress in molecular characterization and targeted therapy provides promising new avenues for treatment, and ongoing research continues to explore ways to improve prevention and management strategies. With continuous efforts in research and clinical practice, the prognosis of cancer endometrial patients is expected to further improve in the coming years.
| Cat. No. | Product Name | Host | Isotype | Application | |
| CABT-L2803 | Mouse Anti-Human PMS2 monoclonal antibody, clone JID523 | Mouse | IgG | IHC | Inquiry |
| CABT-L2858 | Mouse Anti-Human SALL4 monoclonal antibody, clone JID770 | Mouse | IgG | IHC | Inquiry |
| CABT-B739 | Anti-MSH6 (Internal) polyclonal antibody, clone D2D3 | Rabbit | IgG | EMSA, ICC/IF, IHC-P, IP, WB | Inquiry |
| DMAB5373MH | Anti-CCND1 monoclonal antibody, clone EDT-7 | Mouse | IgG2a | IHC | Inquiry |
| DMAB5512MH | Mouse anti-Human MLH-1 Monoclonal antibody, clone H169-16 | Mouse | IgG1 | IHC | Inquiry |
| DMAB5571MH | Anti-ERBB2 monoclonal antibody, clone CW6 | Mouse | IgG | IHC | Inquiry |
| Cat. No. | Product Name | Size | Species Reactivity | Application | Detection Method | |
| DEIA238 | Human Cadherin 1, Type 1, E-cadherin (epithelial), CDH1 ELISA Kit | 5 plates | Human | Quantitative | sELISA | Inquiry |
| DEIA1441 | Mouse DKK1(Dickkopf Related Protein 1) ELISA Kit | 96T | Mouse | Quantitative | sELISA | Inquiry |
| Cat. No. | Product Name | Size | Target | Species | |
| DAG-P0203 | Human CABLES1 peptide | / | / | / | Inquiry |
| DAG-P0087 | Human APC2 peptide | / | / | / | Inquiry |
| DAG-P1291 | Mouse AXIN2 peptide | / | / | / | Inquiry |