Product Overview
The BSA-creatine conjugate is designed with a flexible linker of optimal length and a labeling chemistry that does not interfere with creatine binding. Each lot of the conjugate consists of an optimally loaded BSA with (8-15) creatine molecules per BSA molecule as determined by mass spectrometry.
Molecular Weight
69.7 KDa
Alternative Names
Creatine; BSA Creatine; Creatine BSA
Purity
≥99% conjugates by SEC HPLC
Storage
Recommended long term storage is at -20°C or preferably in a -80°C freezer. The solution may be able to stay at 2-8°C for a few weeks or -20°C for up to 1 year.
Introduction
Creatine is an amino acid that has an important role in cellular energy metabolism. It is present either as a free form or creatine phosphate in mammalian tissues such as liver, kidneys, muscle, brain, and blood. Creatine has been used to treat or prevent several neuromuscular conditions. Immunoassay can be a great method of detecting creatine. However, creatine is difficult to modify due to its intrinsic characteristics. Since Creatine is a very small molecule it is generally very difficult to generate an antibody that binds strongly to the protein for detection.
Keywords
Creatine; BSA Creatine; Creatine BSA
Citations
Have you cited DAGA-186B in a publication?
Let us know and earn a reward for your research.
| Product Name |
Cat. No. |
Applications |
Host Species |
Datasheet |
Price |
Add to Basket |
| Product Name |
Cat. No. |
Applications |
Host Species |
Datasheet |
Price |
Add to Basket |
Primarily synthesized in the kidneys, liver, and pancreas, creatine is a nitrogenous organic acid. After synthesis, creatine is transported to tissues and organs, and creatine phosphate is used as a readily available energy source, especially during the early stages of intense muscle contraction. In skeletal muscle, creatine and creatine phosphate are in equilibrium, with approximately 25% of creatine stored as free creatine and the remainder as creatine phosphate. Creatine is eventually metabolized to creatinine (CRE).
CRE is very stable in the human body, and levels are related to an individual's muscle mass. Serum CRE levels are in the range of 45-90μM in healthy women and 60-110μM in men. CRE levels outside the normal reference range indicate the presence of health problems related to kidney, muscle, and thyroid function, and if they deviate significantly from normal levels, they indicate the presence of very serious diseases such as chronic kidney disease (CKD), various types of muscle disease, cardiovascular problems, and even Parkinson's disease. It has been shown that decreased urinary creatinine excretion in patients with CKD is associated with a high risk of renal failure and death. Since CRE is transported through the blood by the kidneys and excreted in the urine, the clinical focus is on CRE levels in the blood and urine.
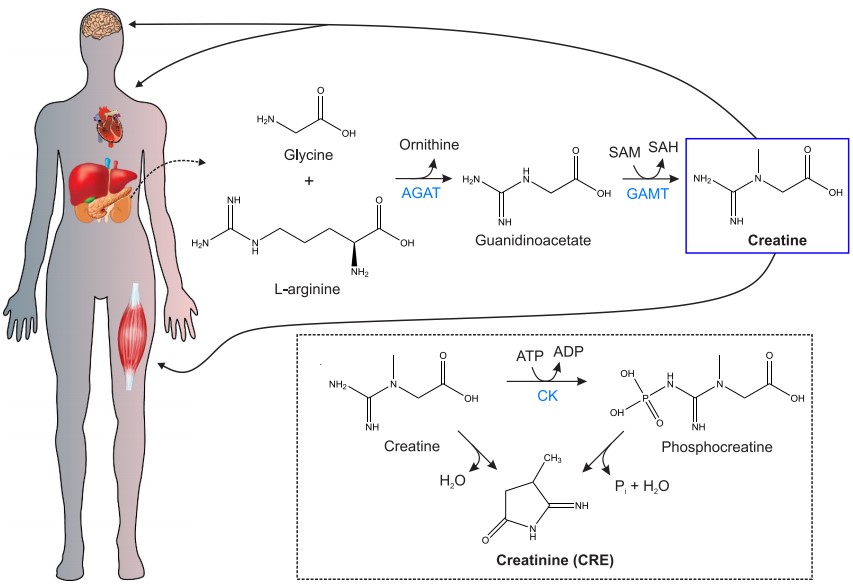 Figure 1. General scheme of the metabolism of Creatine to CRE
Figure 1. General scheme of the metabolism of Creatine to CRE
(Source: Cánovas R, et al. 2019)
However, there are still some physiological factors that limit the application of creatinine as a biomarker. These factors include, but are not limited to, the dependence of serum creatinine levels on hepatic function and skeletal muscle mass, unmeasured and saturable proximal tubular creatinine secretion, the influence of diet, and various forms of extrarenal creatinine clearance. Clinicians must be aware of these limitations. In some cases, clinical adjustments to creatinine-based estimated glomerular filtration rate (eGFR) are necessary. GFR will be overestimated in patients with decreased muscle mass due to advanced age or chronic disease and underestimated in individuals with greater muscle mass or a diet high in cooked red meat. Many medications also interfere with creatinine metabolism or measurement. In addition, renal tubular creatinine secretion increases progressively as GFR decreases and can mask changes in GFR until tubular secretory capacity is saturated, so serum creatinine concentrations may not change until a potential loss of GFR of up to 50% has occurred. The use of serum creatinine to measure GFR in diseases with acute changes in renal function is therefore severely limited.
Alternative Names
CRE
References
1. Cánovas R, et al. Modern creatinine (Bio)sensing: Challenges of point-of-care platforms. Biosens Bioelectron. 2019 Apr 1;130:110-124.
2. Kashani K, et al. Creatinine: From physiology to clinical application. Eur J Intern Med. 2020 Feb;72:9-14.
Q & A
Q: Is DAGA-186B usable in a competitive creatinine ELISA?
A: DAGA-186B is for Lateral flow assay, it should work for competitive creatinine ELISA But not tested yet.
Customer Reviews
Urinary Albumin-to-Creatinine Ratio in Normal Range, Cardiovascular Health, and All-Cause Mortality
JAMA Netw Open
Authors: Mahemuti N, Zou J, Liu C, Xiao Z, Liang F, Yang X.
Abstract
Importance: Although cumulative evidence suggests that elevated urinary albumin-to-creatinine ratio (UACR) in the normal range (<30 mg/g) may be associated with an increased risk of mortality, few studies have investigated whether cardiovascular health (CVH) modifies the harmful outcomes of high-normal UACR.
Objective: To investigate associations of traditionally normal UACR and CVH with all-cause mortality.
Design, setting, and participants: This cohort study used National Health and Nutrition Examination Survey data from 2005 through 2018 and linked mortality information until 2019. Data were analyzed from March 1 through October 31, 2023. The study included adult participants aged 20 to 79 years with a normal UACR (<30 mg/g) based on Kidney Disease: Improving Global Outcomes criteria.
Exposures: The UACR was treated as a continuous variable and categorized into tertiles delineated as low (<4.67 mg/g), medium (4.67-7.67 mg/g), and high (7.68 to <30 mg/g). Cardiovascular health was assessed using Life's Essential 8 scores and grouped as poor (0-49 points), moderate (50-79 points), and ideal (80-100 points).
Main outcomes and measures: Multivariable Cox proportional hazards regression was used to estimate hazard ratios (HRs) and 95% CIs for associations of UACR with all-cause mortality in total participants and as stratified by CVH groups.
Results: The study included 23 697 participants (mean [SD] age, 45.58 [15.44] years; 11 806 women [49.7%] and 11 891 men [50.3%]). During the median 7.8 years (range, 4.5-11.1 years) of follow-up, 1403 deaths were recorded. Near-linear associations were observed for continuous UACR and CVH with all-cause mortality. Compared with the low UACR group, high UACR in the normal range showed an increased mortality risk in the moderate and poor CVH groups (CVH [50-79]: HR, 1.54 [95% CI, 1.26-1.89]; CVH [0-49]: HR, 1.56 [95% CI, 1.10-2.20]), with a significant multiplicative interaction of UACR and CVH (P < .001).
Conclusions and relevance: The findings suggest that high UACR within the normal range is associated with a significantly increased risk of all-cause mortality, with the association more pronounced in adults with poor CVH status. These findings highlight the importance of risk management for early kidney dysfunction, particularly among individuals with poor CVH.
Exploring Renal Function Assessment: Creatinine, Cystatin C, and Estimated Glomerular Filtration Rate Focused on the European Kidney Function Consortium Equation
Ann Lab Med
Authors: Pottel H, Delanaye P, Cavalier E.
Abstract
Serum creatinine and serum cystatin C are the most widely used renal biomarkers for calculating the estimated glomerular filtration rate (eGFR), which is used to estimate the severity of kidney damage. In this review, we present the basic characteristics of these biomarkers, their advantages and disadvantages, some basic history, and current laboratory measurement practices with state-of-the-art methodology. Their clinical utility is described in terms of normal reference intervals, graphically presented with age-dependent reference intervals, and their use in eGFR equations.

