Regulatory status: For research use only, not for use in diagnostic procedures.


| Product Name | Cat. No. | Applications | Host Species | Datasheet | Price | Add to Basket |
|---|
| Product Name | Cat. No. | Applications | Host Species | Datasheet | Price | Add to Basket |
|---|
In recent decades, thousands of new psychoactives have landed in the world's underground illegal market. Often the majority of these drugs are used by criminals for "entertainment" and recreation. To get around the local drug laws, black market illegal drug lords usually extract psychoactives described in the scientific literature and manufactured by big pharma, and make novel psychoactives by tweaking the chemical structure just a bit. In the chemical space, synthetic cannabinoid receptor modulators ("synthetic cannabinoids") have been the leader all along. Synthetic cannabinoids are a category of new psychoactive drugs that behave on the human body like the natural cannabinoid tetrahydrocannabinol (THC). They are used mostly by interacting with the human cannabinoid receptors CB1 and CB2. Synthetic cannabinoids are more powerful pharmacologically in the human body than cannabinoids from nature, and they are more toxic to the human body. Pharmacological effects of synthetic cannabinoids occur via specific mutual tethering with cell membranes. The first cannabinoid receptors were discovered in 1980 and named CB1 (in the order of discovery) and CB2 (the sequence of discovery). CB1 and CB2 are both G protein-coupled receptors, and there is little to distinguish them except in amino acid sequence, signaling mechanism, and tissue distribution. Almost all CB1 receptors are found in the CNS and sometimes also on the dendrites and cell bodies of neurons. Cannabinoids could be modulating different cellular processes by reprogramming the coupling and cell type of CB1 receptors. CB1 receptors expressed on the cell body of the neuron activate Erk and generate brain-derived neurotrophic factor (BDNF). This is how the neuroprotective effect of cannabinoids could be modulated, partly. For instance, mice experiments have demonstrated that when cannabinoids bind to CB2 receptors, immune responses (particularly macrophage-induced helper T cell activation) are altered. Novel cannabinoid compounds keep coming on the market, and the vast majority of them target CB1 receptors. Researchers have discovered that cannabinoids block many neurotransmitters: the CB1 receptor triggered by cannabinoids blocks adenylate cyclase via G protein conduction, decreases cAMP levels, and then cAMP-dependent protein kinase. When protein kinase is disabled, the outward K+ current is amplified; the CB1 receptor is coupled to the Ca2+ channel as well. After the cannabinoids have acted, they lower Ca2+ flow and consequently release neurotransmitters in the presynaptic neurons, before reaching the postsynaptic membrane for either excitatory or inhibitory effects respectively.
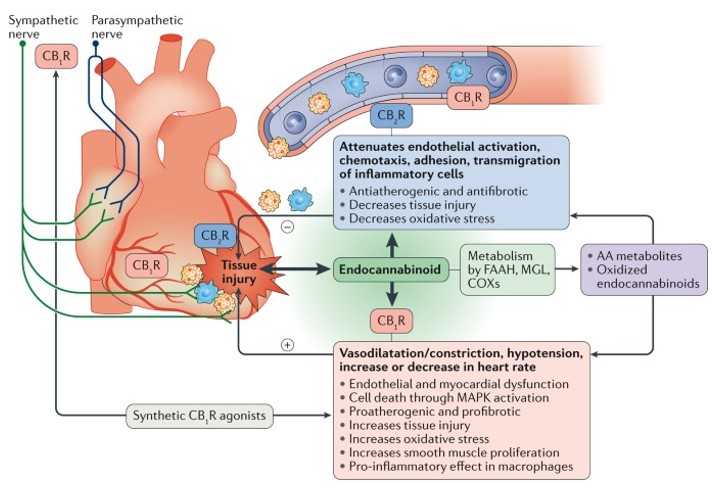 Figure 1: Pathophysiological effects of the endocannabinoid system in health and disease. (Soures: Pacher P, et al. 2018)
Figure 1: Pathophysiological effects of the endocannabinoid system in health and disease. (Soures: Pacher P, et al. 2018)
HU-210, nabilone, dronabinol, etc. have all come out as analogs of 9-THC since 1960. Then came the cyclohexylphenol (CP) family of compounds, with samples that contained synthetic cannabinoids CP-59, CP-47 and their n-alkyl homologues. The first synthetic cannabinoids were a series of naphthoyl indoles – mostly naphthoyl methyl indoles, naphthoyl pyrroles, naphthoyl methyl indole and phenylacetyl indole – invented by Huffman and others in 1994. They were later renamed JWH series compounds (JWH-018, JWH-073 and JWH-200). Synthetic cannabinoids started as naphthoyl indole (JWH-018), progressed to naphthoyl azole (THJ), then indazole (AKB-48), and finally indolecarboxamide (MDMB-CHMINACA). As of the year synthetic cannabinoids first appeared, synthetic cannabinoids are easily divided into two generations. JWH-018 and JWH-250 are first generation; AM-2201 is second generation. In structure, many synthetic cannabinoids aren't any like traditional cannabinoids. The structure puts synthetic cannabinoids roughly into the following groups: naphthoyl indole (JWH-018), naphthylmethyl indole, naphthyl pyrrole, naphthylmethyl indole, phenylacetyl indole (JWH-250), cycloethyl phenol (CP47, 497) and cannabinoids of origin. The bulk of classical cannabinoids are derived from partially reduced diphenylpyran molecules. The core molecule of synthetic cannabinoids has a heterocyclic structure, a substituent, a group between the heterocyclic structure and the substituent, and a side chain. Histochastic shape is indole, indazole, 2-methylindole structure etc.; substituents are mainly lipophilic substituents such as naphthyl, amino acid analogs etc; the substituents are generally amides, carbonyl groups etc; side chains, usually lipophilic side chains, such as pentyl, fluorinated pentyl, p-fluorobenzyl etc. The skin on most synthetic cannabinoids comes from the inside. As mentioned, there are so many different types of synthetic cannabinoids, and the molecular structure of all these synthetic cannabinoids is different, so the detection and tracking of synthetic cannabinoids is an egregious issue. The currently available methods for synthetic cannabinoid molecules detection and characterisation are mostly ELISA, thin layer chromatography, nuclear magnetic resonance (NMR) and infrared (IR), chromatography-mass spectrometry (gas chromatography-mass spectrometry (GC-MS) and liquid chromatography-mass spectrometry (LC-MS)). Of them, the most popular fast and accurate method for synthetic cannabinoids is ELISA as it is simple, straightforward and doesn't require costly instruments and equipment.
Synthetic Cannabinoid Receptor Agonists
Synthetic cannabinoids
Cannabinoid receptor agonists
JWH compounds
CP compounds
AM compounds
HU compounds
RCS compounds
FUBINACA
XLR-11
AB-FUBINACA
References
1. Pacher P, et al. Cardiovascular effects of marijuana and synthetic cannabinoids: the good, the bad, and the ugly. Nat Rev Cardiol. 2018, 15(3):151-166.
2. Roque-Bravo R, et al. Synthetic Cannabinoids: A Pharmacological and Toxicological Overview. Annu Rev Pharmacol Toxicol. 2023, 63:187-209.
![]()