Non small cell lung cancer (NSCLC) is one of the global hot spots in the study of cancer. It is a malignant tumor derived from lung tissue and accounts for about 85% of all lung cancers, making it the most common type of lung cancer. Owing to disparities in smoking prevalence, environmental conditions, and medical quality, the prevalence of non-small cell lung cancer differs across nations. In industrialized countries, where effective anti-smoking campaigns and laws have been implemented, instances of non-small cell lung cancer are gradually dropping. Developing nations, on the other hand, are experiencing an increase in non-small cell lung cancer as smoking rates rise and industrialization accelerates. Tobacco use is the most common cause of NSCLC. Tobacco smoke has a lot of cancer-causing chemicals that can harm your DNA, causing genetic changes and malignancy. The length and quantity of smoking a person smokes are directly linked to the chance of non-small cell lung cancer. Even if you stop smoking for many years, your smoking risk remains high. Lung cancer risk in non-smokers is also significantly increased by exposure to secondhand smoke.
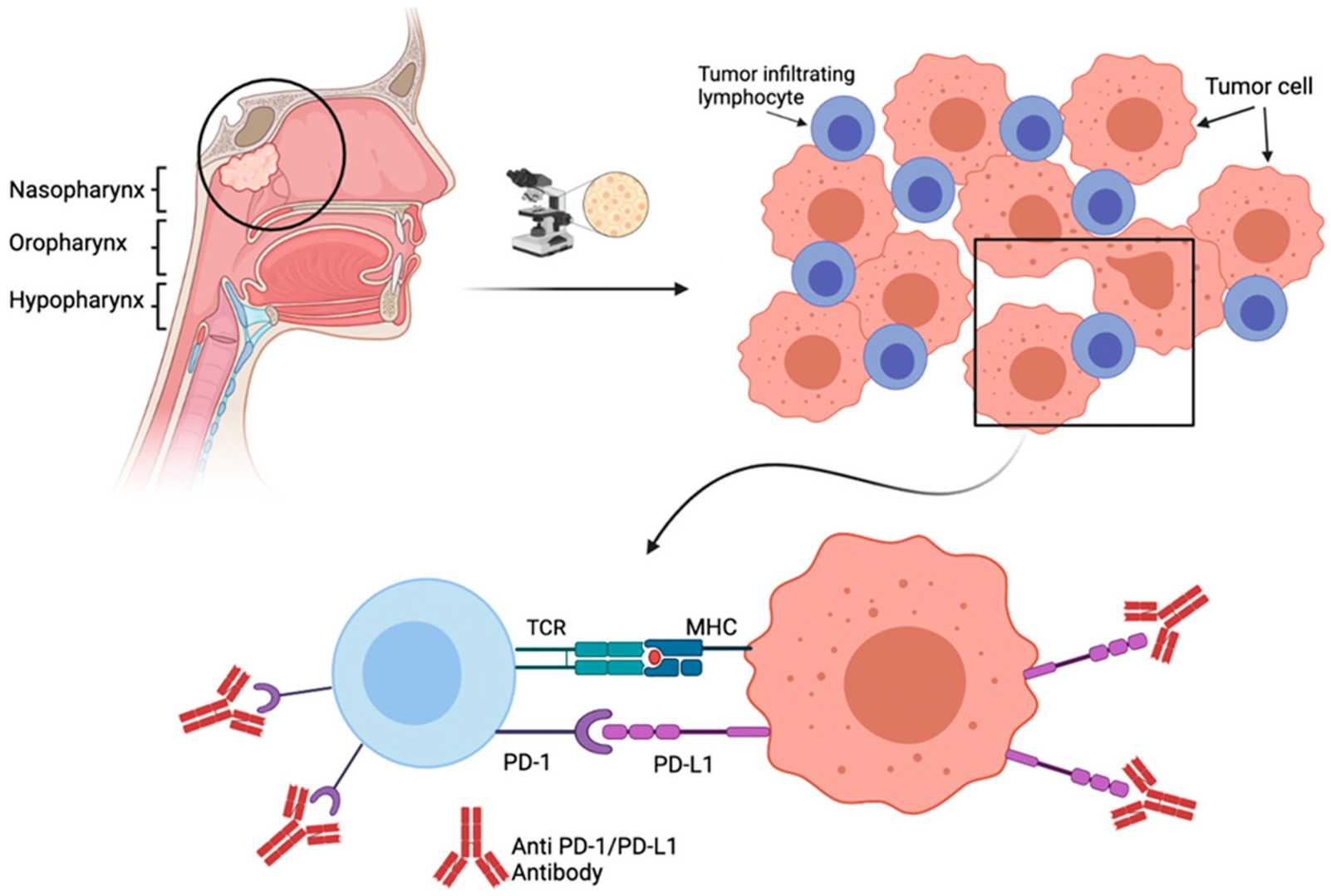 Figure 1. Causal determinants for the possible mechanism of NSCLC development.( Garg, Pankaj, et al. 2024)
Figure 1. Causal determinants for the possible mechanism of NSCLC development.( Garg, Pankaj, et al. 2024)
Pathology and cytology are still considered to be the gold standards for lung cancer diagnosis. Cytological specimens and tissue specimens are all suitable for pathological diagnosis. TTF1 and napsin A are specific indicators for lung adenocarcinoma, and P40, P63, and cytokeratin 5/6 are advised for lung squamous cell carcinoma according to the NSCLC guidelines of the Chinese Society of Clinical Oncology (CSCO). TTF1、P40、P63、 Immunohistochemistry and so on are recommended to be detected, so as to better distinguish between adenocarcinoma and squamous cell carcinoma and other subtypes of NSCLC.
Hereditary genetic mutations are a special risk factor for lung cancer. Studies have shown that approximately 12% -21% of lung cancer cases can be attributed to genetic mutations. Further exploration of genetic mutations may aid in the screening of lung cancer susceptibility genes, as well as the provision of the most effective monitoring techniques for close relatives, based on genetic counseling and clinical diagnosis, to optimize the early detection and prognosis of patients. However, it must be emphasized that the clinical diagnosis and treatment of lung cancer genetic mutations are not a routine method, and there is no need to pay too much attention to them.
Considering the difficulty of obtaining tissue samples, liquid biopsy has developed rapidly. Liquid biopsy has the advantages of safety, non invasiveness, reproducibility, simple performance, and high patient compliance. Circulating tumor DNA (ctDNA) can be used for molecular diagnosis of lung cancer and detection of tumor mutation burden. Especially, there are reports that the genetic mutation results of plasma samples are highly consistent with those of tissue samples.
1. Early symptoms
(1) Chest distension and pain. Early chest pain symptoms in lung cancer are relatively mild, mainly manifested as dull pain, dull pain, and uncertain location. The relationship with breathing is also uncertain. If swelling and pain persist, it indicates that cancer may involve the pleura.
(2) When phlegm blood tumor inflammation leads to necrosis and capillary damage, there may be a small amount of bleeding, often mixed with phlegm, appearing intermittently or intermittently. Many lung cancer patients seek medical attention due to phlegm and blood.
(3) Low fever tumors often have obstructive lung lobes after blocking the bronchi, with varying degrees of severity. Mild cases may only have low fever, while severe cases may have high fever. After medication, there may be temporary improvement, but it will quickly recur.
(4) Cough induced lung cancer, which grows on the bronchial lung tissue, usually produces respiratory irritation symptoms and leads to irritating cough.
2. Late stage symptoms
Patients with advanced non-small cell lung cancer may experience fatigue, weight loss, decreased appetite, and local symptoms such as difficulty breathing, coughing, and hemoptysis.
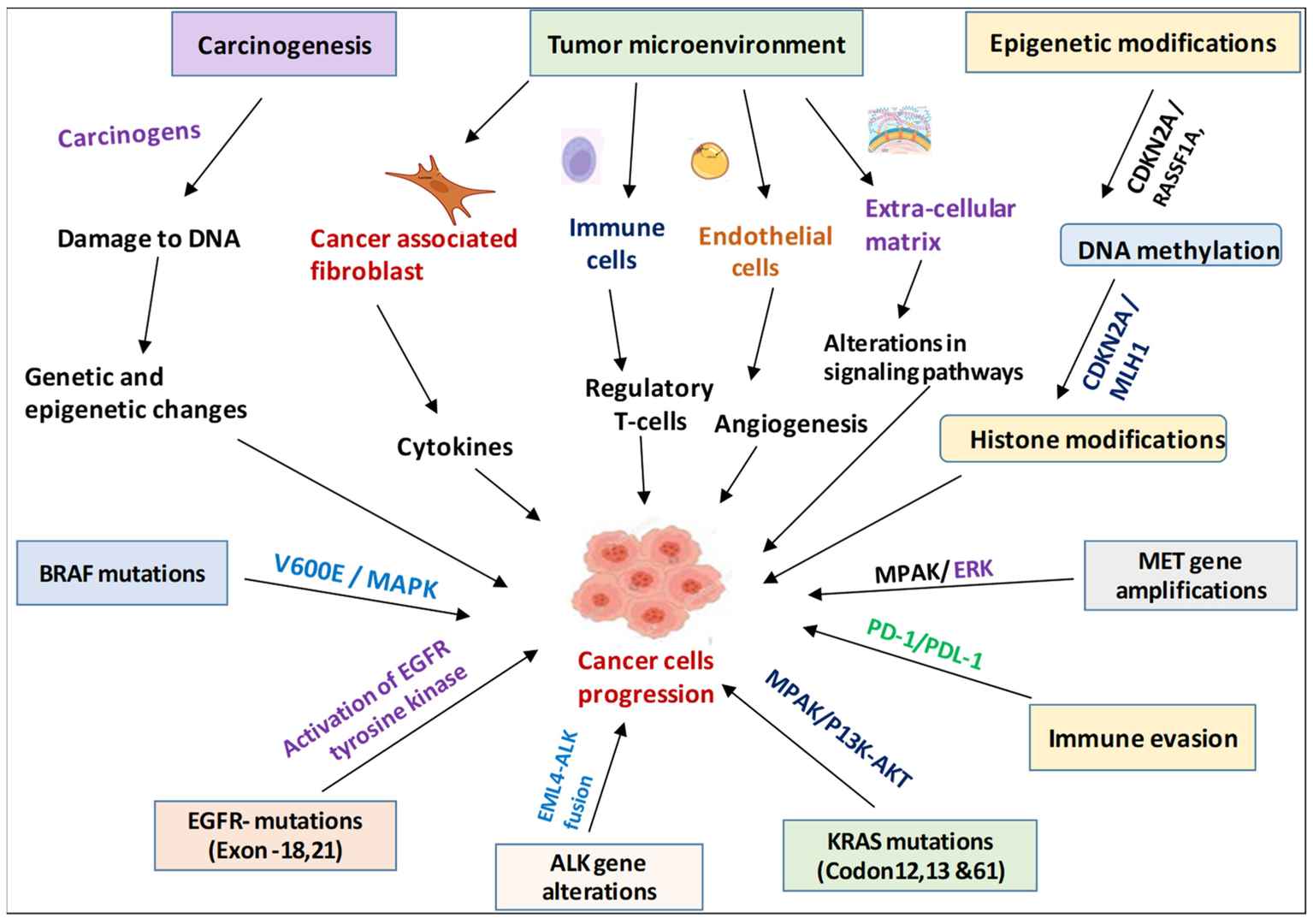 Figure 2. Systematic representation of all advanced techniques for innovative diagnosis and therapy interventions of NSCLC.(Garg, Pankaj, et al. 2024)
Figure 2. Systematic representation of all advanced techniques for innovative diagnosis and therapy interventions of NSCLC.(Garg, Pankaj, et al. 2024)
| Diagnosis | Description |
| X-ray Examination | Through X-ray examination, the location and size of lung cancer can be understood, and local emphysema, atelectasis, or infiltrative lesions or pulmonary inflammatory changes near the lesion may be seen due to bronchial obstruction. |
| Bronchoscopy Examination | Bronchoscopy can directly observe the lesions of the bronchial lining and lumen. Tumor tissue can be used for pathological examination, or bronchial secretions can be aspirated for cytological examination to clarify the diagnosis and determine the histological type. |
| Cytological Examination | Sputum cytology examination is a simple and effective method for the screening and diagnosis of lung cancer, and most primary lung cancer patients can find shed cancer cells in sputum. The positive rate of sputum cytology examination for central lung cancer can reach 70% to 90%, while the positive rate of sputum examination for peripheral lung cancer is only about 50%. |
| Thoracic Exploration Surgery | If the nature of the lung mass cannot be determined through multiple examinations and short-term diagnostic treatment, and the possibility of lung cancer cannot be ruled out, thoracotomy exploration should be performed. This can avoid delaying the condition and causing lung cancer patients to miss the opportunity for early treatment. |
Reference
| Cat. No. | Product Name | Host | Isotype | Application | |
| DPAB-DC3879 | Anti-RIMS2 (aa 181-260) polyclonal antibody | Mouse | WB, ELISA | Inquiry | |
| DPABH-27476 | Anti-RASSF5 (aa 351-400) polyclonal antibody | Rabbit | IgG | WB | Inquiry |
| DPABH-01901 | Magic 6 4 Anti-ALK (Phospho Y158) polyclonal antibody | Rabbit | IgG | IHC-P | Inquiry |
| CABT-L3247 | Rabbit Anti-Human ALK (Phospho-Tyr1096) polyclonal antibody | Rabbit | IgG | IHC, ELISA | Inquiry |
| CABT-L2910 | Mouse Anti-Human CD4 monoclonal antibody, clone JID646 | Mouse | IgG | IHC | Inquiry |
| Cat. No. | Product Name | Size | Species Reactivity | Application | Detection Method | |
| DEIA6310 | CYFRA 21-1 ELISA Kit | 96T | Human | Quantitative | sELISA | Inquiry |
| DEIABL533 | Human soluble Nectin-4 ELISA Kit | 96T | Human | Quantitative | Nectin | Inquiry |
| DEIAZ0030 | Anti-Denosumab ELISA Kit | 96T | Human | Quantitative | sELISA | Inquiry |
| Cat. No. | Product Name | Size | Target | Species | |
| CDBP6013 | RIMS2 blocking peptide | 0.05 mg | Inquiry | ||
| CDBP6014 | RIMS2 blocking peptide | 0.05 mg | Inquiry | ||
| CDBP2485 | Mouse Rassf1 blocking peptide | 100 g | Rassf1 (mouse) | Mouse | Inquiry |
| CDBP2507 | Human RXRB blocking peptide | 100 g | RXR beta | Human | Inquiry |