Syphilis is a chronic and systemic sexually transmitted disease caused by bacteria Treponema pallidum, the Treponema genus is a spirochete bacterium with rich phospholipid membranes and belongs to the spirochaetal order. The only host of Treponema pallidum pallidum (syphilis treponeme) is human, which can cause venereal diseases and congenital diseases. Because its clinical manifestations are highly diverse and can imitate other diseases, it is called a "great imitator". Syphilis was first discovered at the end of the 15th century, spread widely during the Renaissance, and then spread around the world. Its incidence declined in the second half of the 20th century, but since the beginning of the 21st century, the incidence of sexual syphilis in developed countries has increased significantly again.
T. pallidum is a kind of gram-negative bacteria which is famous for its invasiveness and immunity. It has a double-layer membrane structure, but its outer membrane is lack of lipopolysaccharide, and its phospholipid composition is obviously different from that of typical gram-negative bacteria. The lipoproteins expressed by T. pallidum mainly exist below the surface, which can avoid triggering the inherent regulatory mechanism of the host and promote local replication and early transmission. Limited surface antigens can also evade adaptive immunity and increase the survival time in the host.
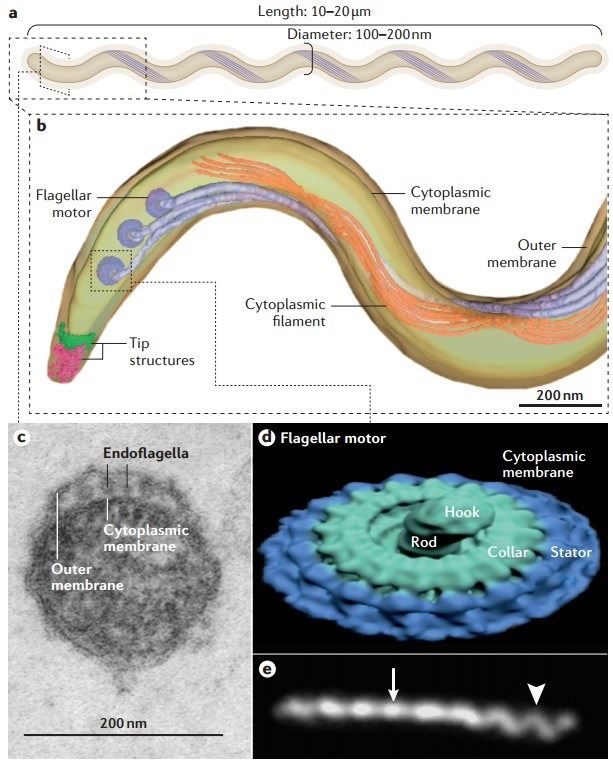 Figure 1. Treponema pallidum
Figure 1. Treponema pallidum
(Source: Peeling RW, et al. 2017)
The origin of syphilis has always been controversial, with several hypotheses attempting to explain it, and although it is impossible to pinpoint the origin of the disease, wars, sea transportation, unstable societies, and sanitary conditions have led to its rapid spread throughout the world. Syphilis was first observed and recorded in 1495, named syphilis in 1521, and began to be monitored in 1941, with the highest number of cases occurring in 1946 (94,957). The incidence of syphilis is still on the rise since 2000, with 6.3 million cases of syphilis recorded annually, and has increased by more than 150% in some high-income countries in the last decade. According to WHO statistics, in 2020 there are a total of 7.1 million adults with syphilis and 661,000 infants with congenital syphilis worldwide.
Syphilis is usually transmitted sexually, but mother-to-child transmission is also possible. Pregnant women are at risk of transmission to the fetus at all stages of syphilis infection, but the risk of infection is higher in the early stages than in the later stages, making optimal and continuous prophylaxis in these patients very important. If left untreated, the disease can go through a series of clinical stages over several years and may lead to irreversible neurological or cardiovascular complications.
The course of an infected person's disease is usually categorized as primary, secondary, latent, and tertiary syphilis with a duration of ≥10 years.
The clinical manifestation of the primary stage of syphilis infection is usually a single, firm, painless, ulcerated hard chancre, which usually appears 2-3 weeks after direct contact with another person's infectious lesion. The hard chancre begins as a maculopapular rash, followed by a papule, and rapidly progresses to an ulcer, which is round or ovoid in shape, with sharp, hardened edges, and pink, red, or gray in color. The primary chancre may be accompanied by tender or non-tender regional lymph node enlargement. If left untreated, the primary lesion subsides spontaneously after 3-6 weeks without scarring. The risk of syphilis transmission after sexual contact is estimated to be about 33%.
Secondary syphilis is the most common clinical symptom. Premonitory symptoms can occur before secondary syphilis, including fatigue, myalgia, sore throat, headache, or low fever. After the hard chancre fades for 3-12 weeks (sometimes at the same time), the blood transmission of spirochetes causes secondary infection.
The rash that secondary syphilis appears can involve both skin and mucous membranes, either localized or widely distributed. It is usually characterized by diffuse macular papules with a diameter of 1cm-2cm, with scaly maculopapular or reddish-brown or "ham-colored" papules on the trunk and extremities, and lesions usually involving the palms of the hands or soles of the feet are diagnostic. Lesions in the palms and feet are usually pink or brown macules or papules. Biett's collarette, a ring of white scaly edges, usually appears on the central surface of the syphilitic papule. At this stage, the lesions mimic any possible morphology, from annular to nodular, lichenoid, or psoriasis-like, so the clinical differential diagnosis may be difficult.
Cutaneous manifestations are often associated with diffuse lymphadenopathy, hepatosplenomegaly, hepatitis, alopecia, osteochondritis, or nephrotic syndrome. The skin lesions of secondary syphilis also do not leave scars, and heal with post-inflammatory hyperpigmentation. With mucosal involvement, the lesions may appear as highly contagious mucosal plaques and sometimes acrodermatitis. Patients may also experience changes in the nails, including brittleness, splitting, onycholysis, onychomadesis, transverse grooves, and Beau lines.
Untreated secondary syphilis takes 4-12 weeks to relieve symptoms. Some high-risk factors (including HIV infection with low CD4 cell count, malnutrition, MSM, previous history of syphilis, diabetes, and alcoholism) may induce lues maligna, which appears as asymmetric ulcers or round necrotic plaques on the scalp, face, trunk, and extremities.
Untreated secondary syphilis is followed by latent infection, which has no clinical manifestations and can only be detected by serological tests. Early latent syphilis can occur between primary and secondary syphilis, or after secondary syphilis has subsided. To distinguish between early and late latencies, CDC established 1 year dividing line that found the highest recurrence rate in the first year after infection (about 25 per cent of patients receiving treatment). At any stage of syphilis, asymptomatic or symptomatic neurologic involvement with abnormal cerebrospinal fluid findings may occur.
Stage III syphilis, also known as late syphilis, is a systemic, multiorgan disease that occurs over years or even decades in about one-third of untreated but infected patients and includes advanced neurosyphilis (generalized paralysis or paralysis of the back), cardiovascular syphilis, or periodontal syphilis. Skin lesions (nodular ulcers or gelatinous lesions) occur in 16% of patients with advanced clinical manifestations; these lesions are usually solitary, unilateral, and asymptomatic.
Gumma is a painless, destructive rubber-like nodule that develops into perforated ulcers several centimeters long, exudates necrotic material, deeply invades tissue and bones, and leaves deep sunken scars after healing. Nervous system involvement of tertiary syphilis is rare due to the presence of antibiotics, but there is also the possibility of meningeal vascular or parenchymal syphilis. Cardiovascular syphilis causes endarteritis, which may lead to aortic aneurysms (usually involving the ascending aorta), aortic valve closure insufficiency, coronary stenosis, and myocarditis. Syphilis during pregnancy carries a significant risk of adverse outcomes, with more than 25% of affected pregnancies ending in stillbirth or spontaneous abortion.
If T. pallidum is transmitted from mother to fetus, congenital syphilis will occur. If the infection spreads within the first trimester of pregnancy, the consequences may include premature delivery, spontaneous abortion, stillbirth, or perinatal death. If the infection spreads in the second to third trimester, most babies born to syphilis mothers appear to be healthy and there is no evidence of clinical or laboratory infection at birth. However, if not treated in time, the disease may appear in a few months to years later.
Thus, congenital syphilis can be categorized into early congenital syphilis (presentation ≤2 years of age) and late congenital syphilis (presentation ≥2 years of age). Symptoms of early congenital syphilis include exfoliative skin rash (syphilitic pemphigus), splenomegaly, adenosis, periostitis, osteochondritis, nephrotic syndrome, pancreatitis, hypophysis (diabetes) and so on. Symptoms of latent congenital syphilis include Hutchinson's teeth, Mulberry molars, interstitial keratitis, mental retardation, hydrocephalus, seizures, optic atrophy, sternoclavicular joint thickening (Higouménakis sign), and clutton joints.
According to the type of syphilis, intramuscular injection of different doses of penicillin G benzathine is still a first-line treatment. At present, penicillin resistance has not been observed in Treponema pallidum. Alternative treatments include oral doxycycline or erythromycin, or ceftriaxone, or intravenous injection. The use of steroids before treatment can avoid immune-mediated self-limited reactions after treatment.
References
| Target | Cat. No. | Product Name | Size | Species | Application | Detection Sample | |
| Syphilis | DEIA2400 | Syphilis (TPA) IgG ELISA Kit | 96T | Qualitative | Serum | Inquiry | |
| DEIA2539 | Syphilis (TPA) IgG/IgM ELISA Kit | 96T | Human | Qualitative | Serum, plasma | Inquiry | |
| DEIA2539NS | Syphilis (TPA) IgM ELISA Kit | 96T | Human | Qualitative and semiquantitative | Serum, plasma | Inquiry | |
| T. pallidum | DEIA069 | Antibody to Treponema Pallidum (Syphilis) ELISA Kit | 96T | Human | Qualitative | Serum, plasma | Inquiry |
| DEIA1795 | Treponema Pallidum IgG ELISA Kit | 96T | Human | Qualitative | Serum | Inquiry | |
| DEIA1855 | Syphilis (Treponema pallidum) Antibody IgG ELISA Kit | 96T | Human | Qualitative | Serum | Inquiry | |
| DEIA2143 | Treponema pallidum Screen ELISA Kit | 96T | Quantitative | Serum, plasma | Inquiry | ||
| DEIA1930 | Treponema Pallidum IgM ELISA Kit | 96T | Quantitative | Serum | Inquiry | ||
| IVDEIA003 | Human anti-TP ELISA Kit | 96T | Human | Qualitative | Serum, plasma | Inquiry | |
| DEIASL2020 | Treponema Pallidum IgG/IgM ELISA Kit | 96T | T. pallidum | Qualitative | Serum, plasma | Inquiry |