The thyroid gland, located in the neck, produces hormones that regulate metabolism. Autoimmune thyroid disease (AITD) is characterized by the presence of antibodies that attack the thyroid's healthy cells, leading to various thyroid disorders. The most common type of AITDs include Graves' disease (GD) and Hashimoto's thyroiditis (HT)(hyperthyroidism in GD and hypothyroidism in HT). Other types include Atrophic thyroiditis and Postpartum thyroiditis. The three most common thyroid autoantibodies are Thyroid peroxidase (TPO) autoantibodies (TPOAb), Thyroglobulin (Tg) autoantibodies (TgAb), and Thyroid-stimulating hormone (TSH) receptor antibodies (TRAb).
Autoimmune thyroid diseases arise due to complex interactions between environmental and genetic factors. Among the major AITD susceptibility genes that have been identified and characterized is the HLADR gene locus, as well as non-MHC genes including the CTLA-4, CD40, PTPN22, thyroglobulin, and TSH receptor genes. The major environmental triggers of AITD include iodine, medications, infection, smoking, and possibly stress. Recent data on the genetic predisposition to AITD lead to mechanisms by which the genetic-environmental interactions may lead to the development of thyroid autoimmunity.
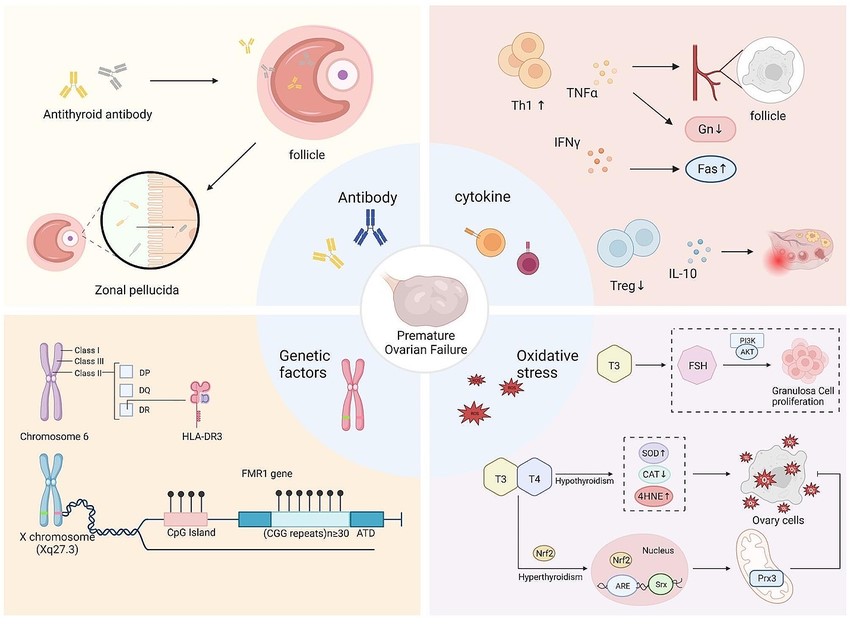 Fig 1. Schematic diagram of the possible mechanism of autoimmune Thyroid disease
Fig 1. Schematic diagram of the possible mechanism of autoimmune Thyroid disease
Autoimmune thyroid diseases are usually accompanied by the presence of anti-thyroid peroxidase (TPO), anti-thyroglobulin (Tg), and anti-thyroid-stimulating hormone receptor (TSHR) antibodies. Antibodies against thyroid antigens such as carbonic anhydrase 2, megalin, T3 and T4, sodium iodide symporter (NIS), and pendrin have also been detected, although rarely.
 Fig. 2 Summary of the immunological mechanisms of AITD leading to HT and GBD
Fig. 2 Summary of the immunological mechanisms of AITD leading to HT and GBD
TPO is responsible for iodine (I2) oxidation and iodination of tyrosyl residues of the Tg molecule. Anti-TPO antibodies from AITD patients can fix complement, destroy thyrocytes, and act as competitive inhibitors of enzymatic activity. It can also act as inductors of oxidative stress. Studies indicated a higher prevalence of IgG1 (70%) and IgG4 (66.1%) forms compared to IgG2 and IgG3. Anti-TPO antibodies are detected in 90–95% of AITD patients, 80% of GD, and 10–15% of non-AITD patients.
Thyroglobulin is a large (600 kDa) glycoprotein consisting of dimers and containing on average 2–3 molecules of T4 and 0.3 molecules T3. The molecule is heterogeneous regarding hormone content, glycosylation, and size. The production of antibodies against Tg can be induced by massive destruction of the thyroid gland. Anti-Tg antibodies do not fix complement because the epitopes are too widely spaced to allow cross-linking. Anti-Tg antibodies in GD belong mainly to the IgG4 class, and IgG2 class is dominant in HT patients. Anti-Tg antibodies are often measured alongside TPOAb to confirm the diagnosis of HT.
The TSHR binds to thyroid-stimulating hormone (TSH), stimulating the production and release of thyroid hormones (T4 and T3) from the thyroid gland. Anti-TSHR antibodies are primarily associated with Graves' disease. TSHR can bedivided to stimulating TSHR antibody and TSH blocking antibody. In addition, neutral antibodies directed against the "hinge" region exist. Anti-TSHR antibodies are found in 90% of GD patients, 0–20% HT, and 10–75% of atrophic thyroiditis patients. The pleiotropic action of anti-thyroid antibodies is typical for anti-TSHR antibodies. Stimulating antibodies is oligoclonal and belong to IgG1 class, while blocking antibodies are polyclonal. Stimulatory antibodies are detected in 73–100% and blocking anti-TSHR antibodies in 25–75% of GD patients.
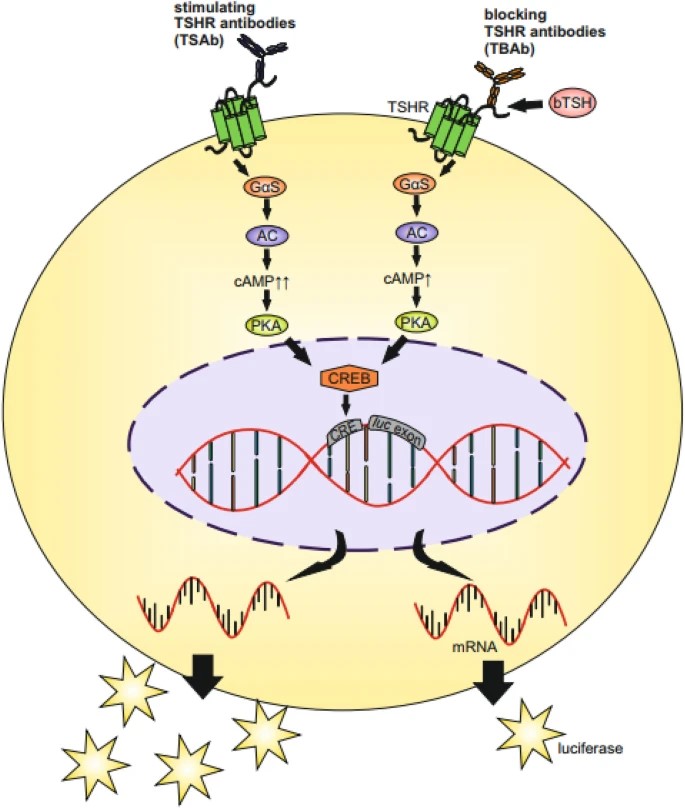 Fig. 3 Schematic of functional cell-based bioassays for anti-TSHR antibodies
Fig. 3 Schematic of functional cell-based bioassays for anti-TSHR antibodies
Autoantibodies plays a fundamental role in the diagnostic approach of autoimmune thyroid disease, and also act as predictors of response to disease treatment.
The presence of thyroid-stimulating immunoglobulins (TSIs) or thyroid receptor antibodies (TRAb) is the hallmark of GBD. The presence of TPOAb and TgAb in the blood is indicative of HT.
Hashimoto's Thyroiditis: Higher levels of TPOAb and TgAb are associated with an increased risk of progression to hypothyroidism, as these antibodies continue to attack and damage the thyroid gland over time.
Graves' Disease: The presence of TSIs or TRAb can predict the likelihood of Graves' disease relapse after treatment, as these antibodies may persist even after treatment to control thyroid hormone levels.
Hashimoto's Thyroiditis: Monitoring levels of TPOAb and TgAb can help assess disease activity and guide treatment decisions. Persistently high antibody levels may indicate ongoing inflammation and thyroid dysfunction.
Graves' Disease: TSIs or TRAb levels can be monitored to assess the effectiveness of treatment in controlling thyroid hormone levels and to detect recurrence of hyperthyroidism.
| Anti-TPO Antibodies | |||
| Cat. No. | Product Name | Application | |
| CABT-L6103 | Human Anti-Human TPO monoclonal antibody, clone D06 | ELISA, Control | Inquiry |
| DMABB-JX374 | Human Anti-Human TPO monoclonal antibody, clone 3H5 | RIA, ELISA, IHC | Inquiry |
| DCAB-TJ171 | Mouse Anti-Human TPO monoclonal antibody, clone C2387N | EIA, ELISA(Detection) | Inquiry |
| DCAB-TJ174 | Mouse Anti-Human TPO monoclonal antibody, clone C2389N | EIA, ELISA(Capture) | Inquiry |
| CABT-Z238R | Rabbit Anti-Human TPO monoclonal antibody, clone CQ7182 | IHC-P | Inquiry |
| CABT-B1771 | Rabbit Anti-Human TPO polyclonal antibody | IHC, ICC | Inquiry |
| DPABH-22989 | Goat Anti-Human TPO polyclonal antibody | WB | Inquiry |
| Anti-TG Antibodies | |||
| Cat. No. | Product Name | Application | |
| CABT-L6107 | Human Anti-Human TG monoclonal antibody, clone D16 | ELISA, Control | Inquiry |
| CABT-L3032 | Mouse Anti-Human?TG?monoclonal antibody, clone JID785 | IHC | Inquiry |
| DCAB-TJ179 | Mouse Anti-Human TG monoclonal antibody, clone Y6F7 | ELISA(Detection) | Inquiry |
| DCAB-TJ180 | Mouse Anti-Human TG monoclonal antibody, clone Y6G0 | ELISA(Capture) | Inquiry |
| CABT-Z234R | Rabbit Anti-Human TG monoclonal antibody, clone CQ7178 | IHC-P | Inquiry |
| DPAB-DC3057 | Mouse Anti-Human TG polyclonal antibody | WB, ELISA | Inquiry |
| DPABH-22038 | Rabbit Anti-Human TG polyclonal antibody | IHC, ICC/IF | Inquiry |
| Anti-TSHR Antibodies | |||
| Cat. No. | Product Name | Application | |
| DMABB-JX42 | Human Anti-Human TSHR monoclonal antibody, clone M22 | FC | Inquiry |
| CABT-L6229 | Human Anti-human TSHR monoclonal antibody, clone 1HA | ELISA | Inquiry |
| CABT-L6230 | Human Anti-human TSHR monoclonal antibody, clone 2HB | ELISA | Inquiry |
| DMABB-JX44 | Human Anti-Human TSHR monoclonal antibody, clone K1-70 | FC | Inquiry |
| DMABB-JX43 | Mouse Anti-Human TSHR monoclonal antibody, clone K1-70 | BL, ELISA, FC | Inquiry |
| DMABB-JX45 | Mouse Anti-Human TSHR monoclonal antibody, clone 5C9 | ELISA, Neut | Inquiry |
| DMABB-JX46 | Mouse Anti-Human TSHR monoclonal antibody, clone K1-18 | ELISA | Inquiry |
| DMABB-JX47 | Mouse Anti-Human TSHR monoclonal antibody, clone 3BD10 | ELISA, FC, IP, WB | Inquiry |
| DMABB-JX48 | Mouse Anti-Human TSHR monoclonal antibody, clone CS-17 | ELISA, FC | Inquiry |