Hepatitis B is a viral infection by hepatitis B virus (HBV) that attacks the liver and can cause both acute and chronic disease. HBV infection usually resolves on its own within 1-6 months and is usually asymptomatic but remains dormant and can be reactivated by immunosuppressive therapy or by treating concomitant viral infections (e.g., hepatitis C). Persistent liver inflammation in patients with chronic hepatitis B (CHB) can lead to fibrosis, cirrhosis, and hepatic decompensation. CHB is also associated with an increased incidence of hepatocellular carcinoma (HCC).
HBV is an enveloped, DNA virus that belongs to the Hepadnaviridae family. The envelope encloses an icosahedral nucleocapsid, which encapsulates a partial double-stranded relaxed circular DNA genome of approximately 3.2 kb. Four partially overlapping open reading frames, termed P (polymerase), S (surface), C (core), and X (HBx protein), define the coding capacity of the HBV genome. Phylogenetic analysis of HBV strains isolated from different regions of the world has identified 10 major genotypes (A-J) that differ by >8% at the nucleotide level of the full-length genome.
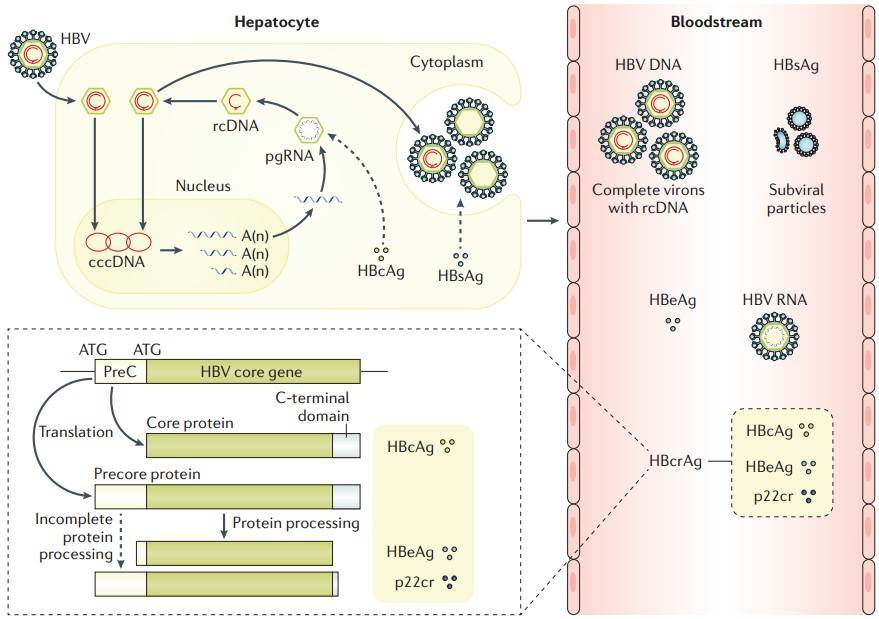 Figure 1. The HBV replication cycle and key viral markers.
Figure 1. The HBV replication cycle and key viral markers.
(Source: Yuen MF, et al. 2018)
The production of excess viral particles (subviral particles or SVP) containing only viral glycoproteins is commonly observed in various viral infections as a common mechanism of immune evasion. In hepatitis B virus infection, spherical particles containing hepatitis B surface antigen (HBsAg) outnumber infectious viruses by 10,000-100,000:1 and inhibit innate and acquired immune responses to varying degrees, playing a major role in chronic HBV infection.
In the open reading frame of the HBsAg gene, three in-frame start codons lead to the production of three isoforms: small (S), medium (M), and large (L). The S-HBsAg region is present in all three isoforms, which contain four transmembrane structural domains (TM 1-TM 4) that drive HBsAg co-translational insertion into the endoplasmic reticulum membrane and the primary antigenic region of HBsAg. M-HBsAg contains an additional amino-terminal structural domain (PreS2), and L-HBsAg contains an additional amino-terminal structural domain (PreS1) on top of M-HBsAg.
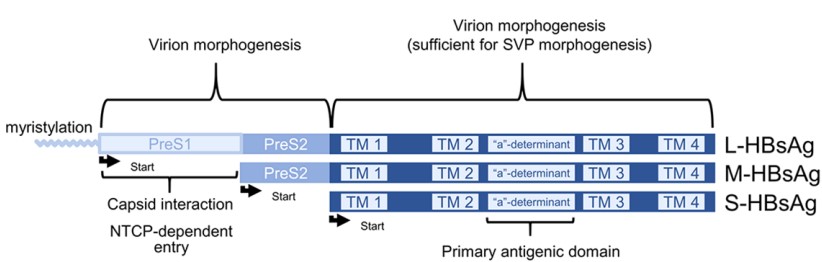 Figure 2. Organization of HBsAg isoforms and their functional domains
Figure 2. Organization of HBsAg isoforms and their functional domains
(Source: Vaillant A. 2021)
HBsAg has a wide range of immunosuppressive properties, and there is sufficient evidence in vitro, in vivo and in humans to show that this characteristic leads to specific dysfunction in the immune response of HBV infection. These immunosuppressive activities include inhibition of innate immunity and suppression or depletion of B and T cell functions.
 Figure 3. HBV-specific immune responses
Figure 3. HBV-specific immune responses
(Source: Yuen MF, et al. 2018)
During infection, the antibody response plays an important role in the clearance of HBV virus particles and infected hepatocytes. In the infected population, patients may naturally clear hepatitis B surface antigen and develop hepatitis B surface antibodies (anti-HBs), while others may progress from chronic hepatitis to liver cirrhosis and hepatocellular carcinoma.
Table 1. Immunoinhibitory Properties of HBsAg
| Immune function | Target of inhibition | Effect observed |
| Innate | TLR function | in vitro, in vivo |
| Cytokine signaling | in vitro, in humans | |
| Monocyte and macrophage function | in vitro | |
| Dendritic cell function | in vitro | |
| NK cell function | in vitro, in vivo, in humans | |
| Adaptive | Sequester anti-HBs | in vitro |
| HBV specific B-cell function | in humans | |
| HBV specific CD4+ T-cell function | in humans | |
| HBV specific T-cell tolerance | in vitro, in vivo | |
| HBV specific T-cell exhaustion | in vivo, in humans |
(Source: Vaillant A. 2021)
HBsAg is the most important marker for the diagnosis of HBV infection, and has become a qualitative diagnostic indicator of hepatitis B virus infection. A number of clinical studies have evaluated the clinical utility of HBsAg and suggested its potential roles, clinical screening of HBsAg is of great significance, which can help us:
Helps in the early diagnosis of hepatitis B. HBsAg appears in the serum of most patients at the end of the incubation period of acute hepatitis B. It reaches a peak in the acute phase and then declines.
Helps in the differential diagnosis of hepatitis B. A person with positive HBsAg is a hepatitis B patient or carrier.
Helps to predict the prognosis of hepatitis B. If HBsAg disappears within 6 months, chronicity does not occur; if HBsAg is persistently positive for more than 6 months, 2/3 of the patients will have prolonged healing and become chronic hepatitis B.
Helps to study the epidemiology of hepatitis B. The most common route of transmission of hepatitis B is mother-to-child transmission at birth (perinatal transmission) or horizontal transmission (exposure to infected blood). Stab wounds, tattoos, punctures, and contact with infected blood and body fluids, such as saliva, menstrual fluid, vaginal fluid and semen, can also spread hepatitis B. The virus may also spread through the reuse of contaminated needles, syringes or sharp objects in medical institutions, communities or people who inject drugs. Sexual transmission is more common in unvaccinated people with multiple sexual partners.
Helps study association of hepatitis B with complications, liver cancer and other diseases. Chronic elevation of HBsAg in vivo is associated with the development of HCC and may be related to chronic endoplasmic reticulum stress-mediated cellular injury or interferon-mediated liver inflammation
Detection of hepatitis B surface antigen in serum is the standard serologic test for confirming hepatitis B virus infection and is also used for screening in population-based epidemiologic studies to determine the prevalence of chronic hepatitis B virus infection. The concentration of HBsAg varies at different stages of the disease, and the concentration of HBsAg is usually higher in individuals who have detected HBeAg.
It is worth noting that when the serum HBV DNA drops to a level that cannot be detected by even sensitive PCR, HBsAg can still be measured. In addition, quantitative detection of hepatitis B surface antigen is of great significance to the prognosis and has been included in the risk score to predict the risk of hepatocellular carcinoma and may also predict the risk of virus rebound after the cessation of nucleotide analogues (NUCs). Positive anti-HBs test results in patients who test negative for HBsAg may be associated with HBV vaccination response, recovery from acute hepatitis, or HBsAg seroconversion in chronic HBV infection.
CHB infection most often occurs in perinatal transmission or very young infection and lasts for several years until the development of hepatitis leads to diagnosis, while mild asymptomatic infection (chronic carrier status) lasts for decades and then reactivated due to changes in the host's immune status. Therefore, the complete elimination of HBV (HBV cure) in patients is still a distant treatment goal. A more realistic goal now is to achieve seroclearance of HBsAg as early as possible after infection (functional cure).
The marker for establishing immune control of hepatitis B virus infection is the removal of HBsAg from the blood. In the absence of treatment, if HBsAg antigen is continuously cleared without detection of the virus and normal liver function, patients are thought to have established a "functional cure" similar to those who have successfully solved their acute hepatitis B virus infection.
Achieving HBsAg clearance during treatment requires effective suppression of circulating HBsAg replenishment from cccDNA and SVP integrated HBV DNA. There are currently two different approaches to accomplish this, targeting HBV mRNA degradation via antisense or RNAi and targeting SVP assembly and release via nucleic acid polymers (NAPs).
The current technology uses triantennary N-acetylgalactosamine conjugate (GalNAc) to enhance the targeting of antisense RNAs and siRNAs to the liver through specific interactions with asialoglycoprotein receptor on hepatocytes. Several GalNAc-antisense and GalNAc-RNAi compounds are currently under clinical evaluation, and these studies have shown that GalNAc-RNAi compounds have very conserved target mRNA/ host protein responses at a variety of different liver targets.
Nucleic acid polymers (NAPs) utilize the sequence independent functionality of phosphorothioate oligonucleotides to interact with exposed amphipathic alpha helices in proteins. In vitro experiments showed that NAPs selectively blocked the assembly and secretion of spherical SVPs without affecting the assembly and secretion of HBeAg or Dane particles. The results suggest that this effect is sequence-independent, thioate-independent, and sugar-modification-independent. However, NAPs treatment is almost universally accompanied by asymptomatic but intense transaminase flares. While these flares appear immune mediated, beneficial and an important component of HBsAg loss during treatment of HBV with approved agents, additional trials in cirrhotic patients will be required established the necessary safety data required to expand NAP-based therapy into this patient group.
References
| Target | Cat. No. | Product Name | Size | Species | Application | Detection Sample | |
| HBsAg | DEIA001 | Hepatitis B Surface Antigen ELISA Kit | 96T | Human | Qualitative | Blood | Inquiry |
| DEIA060 | Antibody to HBsAg ELISA Kit | 96T | Human | Quantitative | Serum, plasma | Inquiry | |
| IVDEIA001 | Human Hepatitis B surface antigen (HBsAg) ELISA Kit | 96T | Human | Qualitative | Serum, plasma | Inquiry | |
| DEIASL263 | Mouse Anti-HBsAg IgG ELISA Kit | 96T | Quantitative | Srerum | Inquiry | ||
| DEIASL271 | Rabbit Anti-HBsAg IgG ELISA Kit | 96T | Quantitative | Srerum | Inquiry |
| Target | Cat. No. | Product Name | Host | Isotype | Application | |
| HBsAg | DPABH-00289 | Anti-HBV type ad, ay Surface Antigen Polyclonal antibody | Goat | IgG | ELISA | Inquiry |
| DPABH-00284 | Anti-HBV type ad, ay Surface Antigen Polyclonal antibody | Rabbit | IgG | ELISA | Inquiry | |
| DCABH-312 | Anti-HBV Surface Antigen Monoclonal antibody, Clone C625N | Mouse | IgG2a | ELISA | Inquiry | |
| DMABT-Z59613 | Anti-HBV type ad, ay Surface Antigen Monoclonal antibody, Clone 98E | Mouse | IgG1 | ELISA, WB | Inquiry | |
| DMABT-Z59614 | Anti-HBV Surface Antigen Monoclonal antibody, Clone UO-3 | Mouse | IgG1, κ | ELISA | Inquiry | |
| DPATB-H81650 | Anti-HBV Surface Antigen Polyclonal antibody | Horse | IgG | Dot, ELISA, IHC-Fr, IP, WB, ICC, IF | Inquiry | |
| DPATB-H81639 | Anti-HBV Surface Antigen Polyclonal antibody | Rabbit | IgG | ELISA | Inquiry | |
| DMAB3544 | Anti-HBV Surface Antigen Monoclonal antibody, Clone A058-17005 | Mouse | IgG2a | ELISA, Pr* | Inquiry |
| Target | Cat. No. | Product Name | Expression System | Tag/Conjugate | Application | |
| HBsAg | DAG-WT366 | Recombinant HBsAg VLP [His] | HEK293 | His | ELISA | Inquiry |
| DAG-WT712 | Recombinant HBV Surface Antigen (Ad/Ay) | P. pastoris | TBD | ELISA, WB | Inquiry | |
| DAG2756 | Recombinant Hepatitis B virus Surface Antigen preS1 | E. coli | Unconjugated | Inquiry | ||
| DAGC278 | Native HBV Surface Antigen (subtype ad) | Human plasma | Unconjugated | Inquiry | ||
| DAG3943 | Recombinant HBV Surface Antigen (subtype ayw) [His] | E. coli | His | WB, ELISA, LFIA | Inquiry | |
| DAG-P2844 | HBV Surface Antigen (full length)(subtype ayw ) | S. cerevisiae | His | SDS-PAGE, ELISA | Inquiry | |
| DAG-P2848 | HBV Surface Antigen (full length)(subtype adr ) | S. cerevisiae | Unconjugated | ELISA | Inquiry |