Gastrointestinal cancer is cancer that develops along the GI tract (also called the digestive tract). The GI tract starts at the esophagus (the tube that takes food from the mouth to the stomach) and ends at the anus (where waste exits the body). Gastrointestinal (GI) cancers are the most predominant malignant type of cancer accounting for 1 in 4 cancer cases and 1 in 3 cancer deaths globally, among which gastric and colorectal cancers are the most common, and other gastrointestinal cancers may occur in the large and small intestines, pancreas, anus, and biliary system.
In the early stages of gastrointestinal cancer, there may be no symptoms. It is almost impossible to feel a GI tumor during development. Therefore, gastrointestinal cancers are often detected on screening or diagnosed after cancer has progressed to the severe stage where it causes symptoms, which may include: abdominal cramps, bloody stools, difficulty swallowing, digestive problems, etc.
The exact cause of gastrointestinal cancer is not fully understood. Generally speaking, gastrointestinal cancers are more likely to develop in men, and the risk increases with age. Studies have linked these cancers to cigarette smoking, alcohol consumption and unhealthy diets.GI tumors may also result from specific underlying conditions. These can include gastroesophageal reflux disease in the esophagus, Helicobacter pylori infection in the stomach, hepatitis B or C virus infection or cirrhosis in the liver. A small percentage of gastrointestinal cancers are inherited.
Mutations in signaling pathways, such as signal transduction systems, are fundamental triggering mechanisms for different types of cancer. Dysregulation of MAPK, Wnt, TGFβ, and JAK-STAT signaling is the most common in gastrointestinal cancer. Wnt signaling pathway, including WISP3 (Wnt1-induced signaling protein 3), APC (adenomatous colonic polyps), β-catenin, AXIN, and TCF4 (T-cell factor 4), plays an important role in carcinogenesis. APC mutation and promoter hypermethylation are two important mechanisms of carcinogenesis and colorectal cancer (CRC) progression. The AXIN genes (AXIN1 and AXIN2) have high mutation frequencies in CRC cases. The transformation of EGFR and its downstream pathway mediators mediates the development of gastrointestinal cancers. E-cadherin (cdh1) mutations cause a specific type of gastric cancer called hereditary diffuse gastric cancer. Additionally, VEGF pathway, HGF/MET signaling pathway, Hippo pathway, and Notch signaling are also involved in gastrointestinal cancers. Moreover, tumour growth is not solely driven by tumour cell-intrinsic mechanisms, but also depends on paracrine signals provided by the tumour micro-environment. In GI cancer are composed of highly complex tissue and most of these tissues are constantly replenished by the proliferation and differentiation of multi-potent tissue stem cells. These processes are regulated by paracrine signals provided by cells of the stem cell niche. Such as members of the A disintegrin and metalloprotease (ADAM) family are involved in all these processes, playing a decisive role in gastrointestinal tumorigenesis.
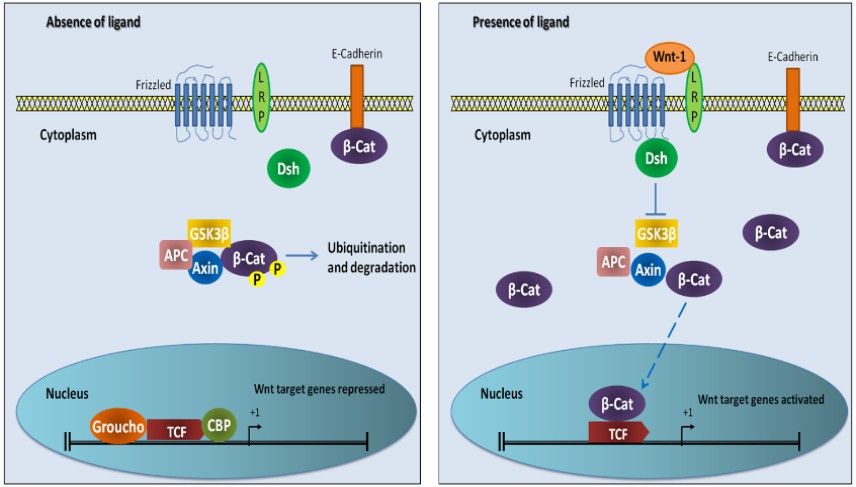 Fig. 1 The Wnt signaling pathway
Fig. 1 The Wnt signaling pathway
The methods that are most usually used in diagnostic tests for gastrointestinal cancer include colonoscopy, endoscopy, tissue biopsy, and imaging. In addition, a variety of biomarkers can also be applied to the auxiliary diagnosis and prognosis of gastrointestinal cancer. For example, IGFBP2 is involved in the proliferation, migration, and invasion of cancer cells and has been used for early detection and assessment of progression in colorectal cancer. ESM1, CTHRC1 and AZGP1 have been shown to be effective and significant for the diagnosis of colorectal cancer. For gastric cancer, biomarkers applied in clinical practice include AFP, CEA, CA19-9, CA72-4 and CA12-5, among which, CEA and CA19-9 are commonly used as prognostic markers. Additionally, Potential immune-related prognostic biomarkers for gastric cancer, includes INHBA, ANGPTL1, ACKR1, GHR, etc.
Treatment modalities for gastrointestinal cancer include surgery, chemotherapy, and radiation therapy. Of these, surgery is the most common treatment. At the same time, for the various signaling pathway targets in the occurrence and development of gastrointestinal cancer, a variety of targeted drugs have been used in the treatment of gastrointestinal cancer, such as
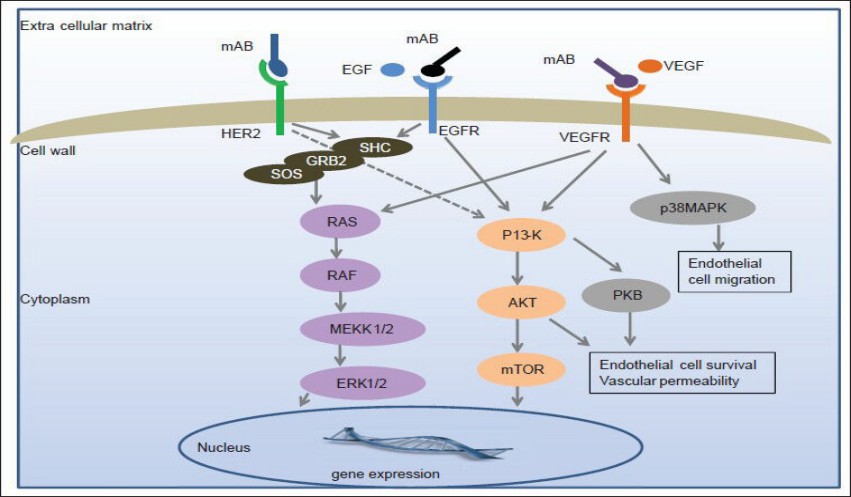 Fig. 2 Molecular targets and signaling pathways of targeted treatment for gastrointestinal cancers
Fig. 2 Molecular targets and signaling pathways of targeted treatment for gastrointestinal cancers