Multiple myeloma (mm) is a malignant proliferative disease of plasma cells. There is no common alias for this disease. It is characterized by uncontrolled proliferation of plasma cells in the bone marrow and the secretion of monoclonal immunoglobulin, which eventually causes damage to organs or tissues. The incidence of this disease in men is higher than that in women. The incidence of mm is lower than that in western countries, but it increases year by year, and there is a certain genetic correlation. The risk of mm in the immediate family members of patients is higher. The mortality and prognosis were significantly different, and the median survival time was about 3-4 years.
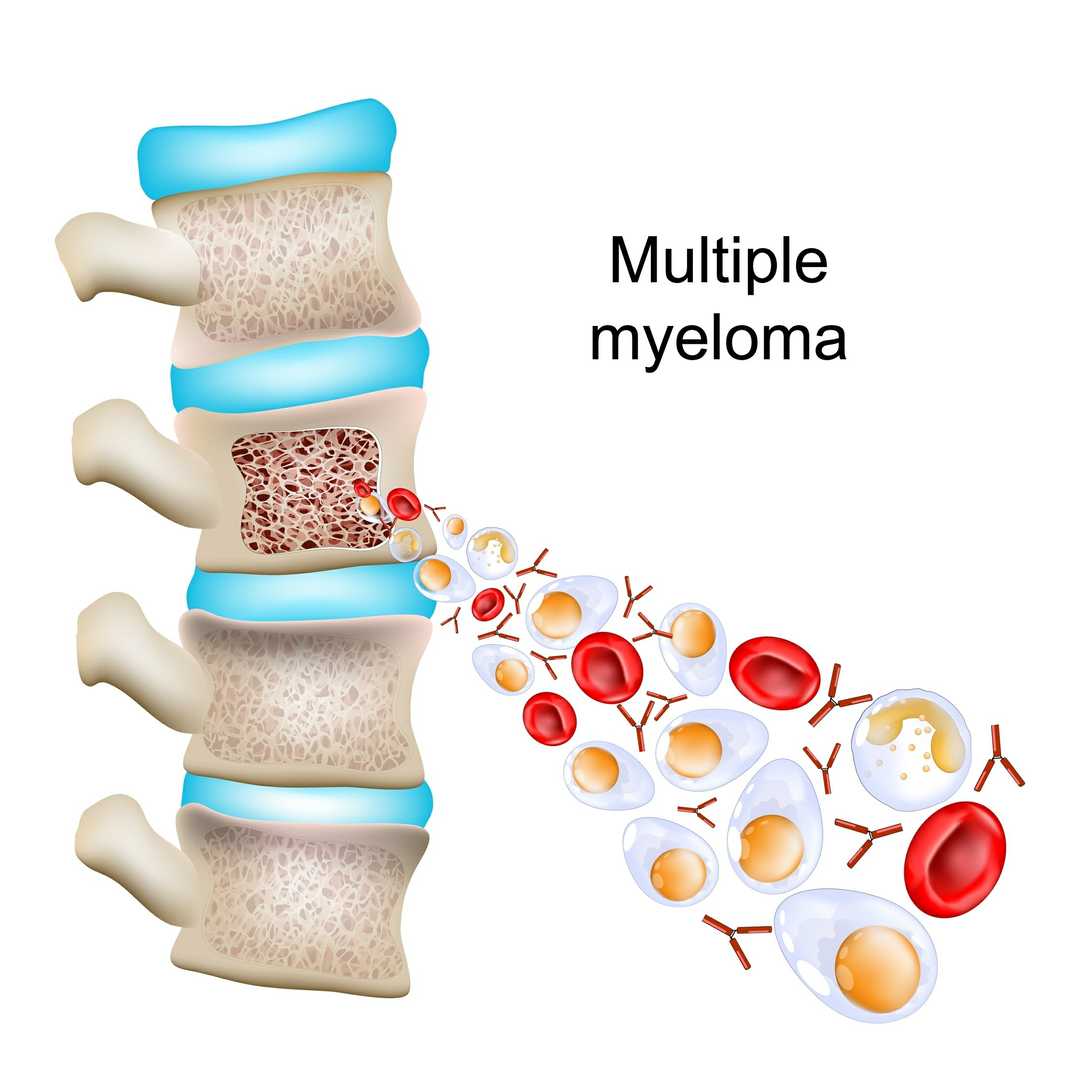 Figure 1. Multiple Myeloma.
Figure 1. Multiple Myeloma.
The clinical symptoms of multiple myeloma are diverse, and the most classic quadruple sign (crab) is: elevated blood calcium, renal dysfunction, anemia, bone pain. Other symptoms include paresthesia, hepatosplenomegaly, lymphadenopathy, fever, etc. Bone pain is often chest pain and low back pain, with obvious symptoms after exercise. It is worth noting that multiple myeloma is not an infectious disease and is not infectious. The treatment of multiple myeloma is not limited to, but generally includes general treatment, drug treatment, surgical treatment, etc. General treatment includes the use of bisphosphonates to control bone destruction, active calcium reduction to treat hypercalcemia, dialysis to treat end-stage renal failure, etc. The use of bortezomib, lenalidomide and other chemotherapeutic drugs are common methods of drug treatment, and the treatment plan should be individualized according to the patient's disease condition and physical condition. In addition, for patients who are suitable for it, autologous hematopoietic stem cell transplantation can also be performed. Surgical treatment is mainly used for the treatment of pain that cannot be controlled by drug methods and the treatment of extramedullary infiltration foci of myeloma. The prognosis is different due to individual differences, but recurrence is inevitable, and follow-up is required.
Multiple myeloma mostly occurs in middle-aged and elderly people, with obvious differences in gender distribution. The proportion of men is higher than that of women. Previous data showed that the incidence of mm was about 1.0/100000, which was lower than that in western countries, but it had an increasing trend year by year. The incidence of multiple myeloma has a certain genetic correlation, and the risk of patients' immediate family members is higher than that of the general population.
According to the type of immunoglobulin secreted by myeloma cells, the disease can be divided into the following types: IgG type, IgA type, IgD type, IgM type, IgE type, light chain type, double clone type and non secretory type. It can also be further divided into κ type and λ type according to the light chain type. The clinical staging criteria of multiple myeloma include the traditional Durie salmon (D-S) staging system, the international staging system and the revised international staging system. Although the clinical items of staging are different, they are all divided into stages I, II and III according to the severity. In the D-S stage, according to whether the renal function is normal or not, it is divided into subtypes A and B.
There are great differences in the course of multiple myeloma. Some patients can live more than 10 years, but the median survival time is 3-4 years. The median survival time is half of the survival time, which means that only 50% of individuals can survive this time.
At present, it is not clear. However, molecular and cellular genetic abnormalities are closely related to the pathogenesis of multiple myeloma. Radiation exposure, viral infection and exposure to certain chemicals are considered to be involved in the pathogenesis of multiple myeloma, but there is no direct evidence.
The risk factors related to the incidence of MM are still unclear. Epidemiological data show that the incidence of MM is related to gender, age and race. Occupational environment, lifestyle, ionizing radiation, exposure to chemical poisons, chronic antigen stimulation, autoimmune diseases, drugs, viral infection, etc. may be involved in the pathogenesis of mm, and the specific mechanism is still controversial.
The symptoms of multiple myeloma are diverse, but the most classic quadruple sign (crab) is elevated blood calcium, renal dysfunction, anemia, bone pain. Other symptoms are paresthesia, hepatosplenomegaly, lymphadenopathy, fever, etc.
Typical symptoms
| Symptoms | Descriptions |
| Medical Examination | For patients suspected of multiple myeloma, doctors will pay attention to whether there is superficial lymphadenopathy, whether there is tongue hypertrophy, and whether there is tenderness in the spine and vertebral body. |
| Imaging examination | Including whole-body x-ray (including skull, pelvis, femur, humerus, thoracic vertebra, lumbar vertebra, cervical vertebra), CT or magnetic resonance imaging (whole-body or local, including cervical vertebra, thoracic vertebra, lumbosacral vertebra, skull) and pet/ct. |
| Pathological examination | Patients with suspected amyloidosis need to complete abdominal wall fat, bone marrow or affected organ biopsy, and Congo red staining. |
| Symptoms | Descriptions |
| Acute Phase Treatment | Some patients have pathological fractures due to tumor cell infiltration, osteolytic lesions, etc., or neurospinal cord compression symptoms due to tumor compression of spinal cord or nerve, or even paraplegia. For example, when paraplegia occurs, emergency surgery is often needed first to restore spinal homeostasis and relieve the corresponding clinical symptoms caused by nerve or bone marrow compression. |
| General Treatment | Oral or intravenous bisphosphonates are recommended for bone disease patients to control bone destruction. Patients with severe hypercalcemia should be actively treated with calcium reduction, mainly through hydration, alkalization and diuresis. Drug treatment includes the use of high-dose glucocorticoids, bisphosphonates and calcitonin. Patients with end-stage renal failure should be actively dialyzed, and patients with chronic renal insufficiency need to start non dialysis treatment in time. |
| Surgical Treatment | Patients with pathological fractures of long bones and vertebral compression fractures need orthopedic fixation surgery or bone cement treatment. |
| Cat. No. | Product Name | Host | Isotype | Application | |
| DPAB-DC3898 | Anti-DAZAP2 (aa 93-168) polyclonal antibody | Mouse | / | WB, ELISA | Inquiry |
| DPAB-DC3317 | Anti-ZKSCAN3 (aa 431-536) polyclonal antibody | Mouse | / | ELISA | Inquiry |
| DPABH-08116 | Anti-TRAPPC1 (full length) polyclonal antibody | Mouse | IgG | WB | Inquiry |
| Cat. No. | Product Name | Size | Species Reactivity | Application | Detection Method | |
| DEIA4632 | Human Immunoglobulin Free Light Chains Kappa and Lambda ELISA Kit | 2 96T | Human | Quantitative | sELISA | Inquiry |
| DEIASL022 | Anti-Tocilizumab ELISA Kit | 96T | / | Quantitative | / | Inquiry |
| DEIA-LL167 | Human IRF4 ELISA Kit | 96T | Human | Quantitative | sELISA | Inquiry |
| DEIA-XYA1064 | IRF4 ELISA Kit | 96T | Human, Mouse | Qualitative | Inquiry |
| Cat. No. | Product Name | Size | Target | Species | |
| DAG-WT1170 | Human Bence Jones Kappa Light Chain protein | 1 mg | Bence Jones protein | / | Inquiry |
| DAG-WT670K | Val-Cit-PAB-MMAE [KLH] | 1 mg | MMAE | / | Inquiry |
| DAG-WT670B | Val-Cit-PAB-MMAE [BSA] | 1 mg | MMAE | / | Inquiry |
| DAG-WT678K | Mc-MMAF [KLH] | 1 mg | MMAF | / | Inquiry |
| DAG-WT678B | Mc-MMAF [BSA] | 1 mg | MMAF | / | Inquiry |
| DAG-WT679K | MC-Val-Cit-PAB-MMAF [KLH] | 1 mg | MMAF | / | Inquiry |
| DAG-WT679B | MC-Val-Cit-PAB-MMAF [BSA] | 1 mg | MMAF | / | Inquiry |