Cholangiocarcinoma which people know as bile duct cancer represents a rare yet aggressive type of cancer that begins in the bile ducts. The digestive system relies on these narrow tubes because they transport bile from both the liver and gallbladder to the small intestine. While cholangiocarcinoma remains a rare disease worldwide its regional incidence shows substantial variation with certain Southeast Asian areas displaying elevated rates because of particular risk factors. Due to its stealthy progression cholangiocarcinoma frequently leads to advanced stage diagnosis. Detecting the disease at a late stage creates major obstacles for effective medical intervention which emphasizes the need to comprehend its complex characteristics.
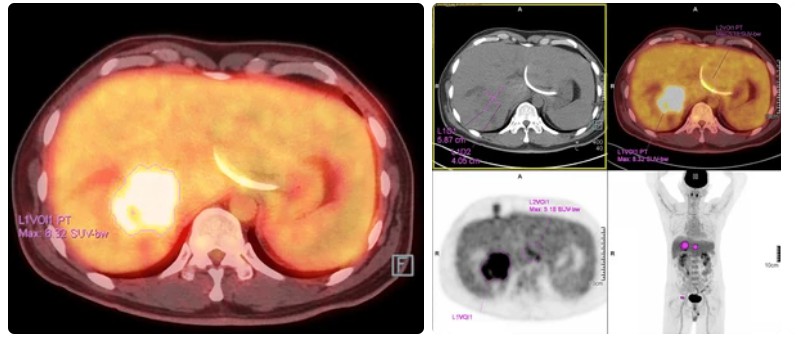 Figure 1. Cholangiocarcinoma.
Figure 1. Cholangiocarcinoma.
The etiology of cholangiocarcinoma is still unclear. May be related to the following factors:



Patients might suffer from persistent jaundice without pain which progressively deteriorates and commonly presents with itching skin and weight reduction.
While middle and lower bile duct cancer patients might show gallbladder enlargement upon palpation and Murphy's sign testing negative, hilar cholangiocarcinoma patients typically do not exhibit gallbladder enlargement.
The stool looks grayish white with a white clay appearance. Bile duct cancer commonly obstructs flow into the duodenum leading to clay colored stool because bile cannot reach this part of the small intestine. Patients with bile duct cancer usually have dark yellow urine, similar to strong tea.
Ascites and lower limb edema can occur in patients experiencing decompensated liver function. Compression or invasion of the portal vein by tumors leads to portal hypertension while late-stage patients may develop hepatorenal syndrome.
The levels of blood total bilirubin, direct bilirubin, alkaline phosphatase, and gamma glutamyltransferase show significant elevation. Doctors can identify this condition by noticing the mild abnormalities in transaminase levels alongside alterations in bilirubin which help differentiate from viral hepatitis. Abnormal liver function in patients can lead to extended prothrombin time measurements. Elevated levels of CA19-9 and CEA can be present in certain patients.
B-ultrasound examination is simple, fast, accurate, and cost-effective, and can detect: Ultrasonic imaging examination detects duct dilation throughout the liver and outside the liver and shows the exact location of biliary blockages while determining the kind of obstruction. In cases of obstructive jaundice the preferred diagnostic tool is an ultrasound examination. Endoscopic ultrasound avoids interference from intestinal gas while its high frequency ultrasound probe displays extrahepatic bile duct tumors with greater clarity. The technique accurately assesses the invasion depth in middle and lower bile duct tumors as well as hilar bile duct cancers and identifies regional lymph node metastasis. By using ultrasound guidance medical professionals can perform cholangiography directly and extract bile through a puncture technique to assess CA19-9 and CEA levels while also conducting bile cytology examinations. Under ultrasound direction doctors can puncture pathological tissue to perform histological examination.
PTC provides clear visualization of the morphology and distribution of bile duct obstructions in both intrahepatic and extrahepatic regions. This procedure requires invasive intervention and patients often face severe complications such as postoperative bleeding and bile leakage.
CT imaging provides precise information about the location and size of bile duct dilation and blockages and accurately identifies lesion characteristics. Three dimensional spiral CT cholangiography (SCTC) shows potential to replace PTC and ERCP examinations.
MRCP examination functions as a non-invasive technique for biliary imaging. The imaging examination method known as MRCP stands as the preferred choice for inspecting hilar cholangiocarcinoma because it produces comprehensive visualizations of intrahepatic bile ducts along with tumor obstruction locations and extents while revealing liver parenchymal invasion or metastasis presence.
Dynamic images of the biliary tract are captured through intravenous injection of 99mTc EHIDA followed by continuous gamma camera imaging.
We aim to analyze how portal vein and hepatic artery interact with tumors to evaluate tumor resectability before surgery. Digital subtraction angiography (DSA) shows how hepatic portal blood flow interacts with tumors which helps in planning radical surgery for cholangiocarcinoma.
Medical professionals diagnose cholangiocarcinoma through clinical examination together with laboratory tests and imaging techniques and histopathological evaluation.
Laboratory Tests
Biopsy and Cytology
Staging and Prognosis
Patient management strategies demand evaluation of tumor stage and location in addition to the patient's fitness level.
| Treatment Strategies | Descriptions |
| Surgical Resection |
|
| Liver Transplantation | Patients who have early-stage pCCA and PSC qualify for liver transplantation if they meet strict criteria such as those established by Mayo Clinic. |
| Systemic Therapy |
|
The battle against cholangiocarcinoma will see major advancements only when early detection methods improve alongside personalized medical treatments and innovative therapies. Surviving cholangiocarcinoma requires a comprehensive support system. Patients need to utilize available resources, maintain communication with their care team, and prioritize quality of life to effectively manage this complex disease.
| Cat. No. | Product Name | Host | Isotype | Application | |
| DCABH-200434 | Anti-DBNDD2 monoclonal antibody | Rabbit | IgG | WB, ELISA | Inquiry |
| DCABH-200761 | Anti-AJUBA monoclonal antibody | Human | IgG | WB, ELISA | Inquiry |
| DCABH-201611 | Anti-SLC35G2 monoclonal antibody | Rabbit | IgG | WB, ELISA | Inquiry |
| DCABH-201667 | Anti-TUBB4B monoclonal antibody | Rabbit | IgG | WB, ELISA | Inquiry |
| DCABH-201740 | Anti-ZCCHC9 monoclonal antibody | Rabbit | IgG | WB, ELISA | Inquiry |
| DPABH-13187 | Anti-ZCCHC9 (aa 214-263) polyclonal antibody | Rabbit | IgG | WB | Inquiry |
| DPABH-20512 | Anti-RPL4 polyclonal antibody | Rabbit | IgG | IHC-P, ICC/IF | Inquiry |
| Cat. No. | Product Name | Size | Target | Species | |
| CDBP0804 | Mouse Cideb blocking peptide | 50 g | CIDE B | Mouse | Inquiry |
| CDBP1106 | Human EIF5A blocking peptide | 100 g | eIF5A | Human | Inquiry |
| CDBP2309 | Human RAD51AP1 blocking peptide | 100 g | PIR51 / RAD51AP1 | Human | Inquiry |
| CDBP2693 | Human SLAIN2 blocking peptide | 100 g | SLAIN2 | Human | Inquiry |