The pancreas is a small hockey-ball-shaped gland located behind the stomach. The main job of the pancreas is to help digest food and regulate blood sugar levels over the body. Pancreatic cancer occurs when cells in the pancreas mutate, start multiplying out of control and form a malignant mass. Pancreatic cancer is one of the common malignant tumors of digestive tract. Due to its insidious and atypical clinical symptoms, diagnosis and treatment are quite difficult, which makes it ranked as the 7th cause of cancer mortality worldwide. There are two types of tumor growth in the pancreas: exocrine and neuroendocrine. About 93% of pancreatic tumors are exocrine, and the most common type is called adenocarcinoma and generally begins in the pancreatic duct. The remaining pancreatic tumors (about 7% of the total) are neuroendocrine tumors (NETs), also known as pancreatic NETs (PNETs).
There are currently no confirmed causes of pancreatic cancer. But there are risk factors such as smoking, obesity, diabetes.Additionally, pancreatic cancer is with family history and genetic susceptibility: people with family risk factors have a nine-fold higher risk of pancreatic cancer than those without a family history. In familial pancreatic cancer, BRCA2 and PALB are the most common mutations.
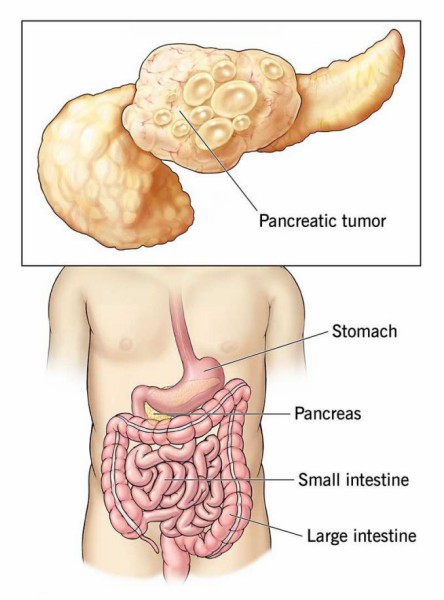 Fig 1. Pancreatic tumor and the location of pancreas
Fig 1. Pancreatic tumor and the location of pancreas
Occurrences of pancreatic cancer are involved in at least 12 different core signaling pathways that were altered in 67-100% of the tumors. The most commonly observed signature genetic lesions in pancreatic cancer are kirsten rat sarcoma viral oncogene homolog (K-Ras), P16/ cyclin-dependent kinase inhibitor 2A (CDKN2A), tumor protein P53 (P53), breast cancer 2 early onset (BRCA2) and SMAD family member 4 (SMAD4)/ deleted in pancreatic carcinoma 4 (DPC4) 6. In pancreatic cancer patients, K-Ras mutations are often considered as an initiating event occurring in adult cells, soon followed by mutation to P16 and later P53 and SMAD4 loss.
 Fig 2. Pancreatic precursor lesions and genetic events involved in pancreatic adenocarcinoma progression
Fig 2. Pancreatic precursor lesions and genetic events involved in pancreatic adenocarcinoma progression
Non-invasive imaging techniques and endoscopic ultrasonography are commonly used in the diagnosis of pancreatic cancer. Secretin enhanced magnetic resonant imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) have been shown to have a good to excellent concordance with endoscopic ultrasound (EUS) findings when used as a one-time screening modality and avoids the risk of ionising radiation. However, EUS has a higher sensitivity for identifying solid pancreatic lesions, less than 2cm, when compared to CT and MRI. EUS is also able to identify worrisome features in pancreatic cysts and can be combined with fine needle aspiration cytology to help further characterise these lesions. The combination of EUS and MRI/MRCP is the imaging modality recommended by the International Pancreatic Cancer Screening Consortium.
Furthermore, the investigation of potential biomarkers, including liquid biopsies, to aid in pancreatic cancer screening, diagnosis, and treatment has been an area of intensive research. Currently Serum CA 19-9 is the only FDA approved biomarker recommended for pancreatic ductal adenocarcinoma (PDA). Over 2,000 biomarker studies related to pancreatic cancer appear in the literature, highlighting the need to discover and develop improved tests. Such as ApoA1, CA125, CA19 -9, CEA, ApoA2 and TTR used for the early detection of PDAC; the combination of serum CA19-9, CA125, and CEA used to identify subgroups of patients who would benefit from adjuvant chemoradiotherapy. A wide range of biomarkers are also applied to pancreatic cancer prognosis as SMAD4, angiogenic markers (eg, PDGF, MMP, VEGF), inflammatory markers (neutrophil-to-lymphocyte ratio, NLR), immune markers (associated with poorer prognosis: FOXP3, CD68, CD163, CD204 and CD66b; associated with improved prognosis: CD3, CD8, CD4, CD20).
Treatment for pancreatic cancer depends on a variety of factors, including where the tumor is, what stage it is, the patient's health, and whether the cancer has spread beyond the pancreas.
Surgical resection is the only curative treatment for pancreatic cancer, and the addition of chemotherapy (eg, gemcitabine, FOLFIRONOX) in the adjuvant setting has been shown to improve survival. There are some optimistic results suggesting that the use of chemoradiotherapy in the neoadjuvant setting can further improve survival. In addition, targeted therapy and immunotherapy are also commonly used in the treatment of pancreatic cancer such as EGFR inhibitor erlotinib, PARP inhibitor Lynparza, NTRK inhibitors Larotrectinib (Vitrakvi) and entrectinib (Rozlytrek), CTLA-4 antagonizer Ipilimumab.