Human papillomavirus (HPV) is a spherical DNA virus that is widely present in nature and serves as the sole host for humans. It is highly tolerant to dryness and can be stored for a long time. Currently, there are only over 150 known subtypes of HPV, which can be classified into low-risk and high-risk types based on the severity of the diseases they cause. The clinical symptoms of the disease include various types of skin warts, such as common warts, flat warts, plantar warts, etc. In addition, high-risk HPV can cause various tumors, such as cervical cancer, anal cancer, penile cancer, etc. The main transmission routes include contact transmission, sexual transmission, and mother to child transmission, with sexual contact being the most common route of infection. People with HPV are generally susceptible, but those with premature sexual intercourse, hormonal imbalances, weakened immunity, multiple sexual partners, smoking, and other factors are more likely to be infected.
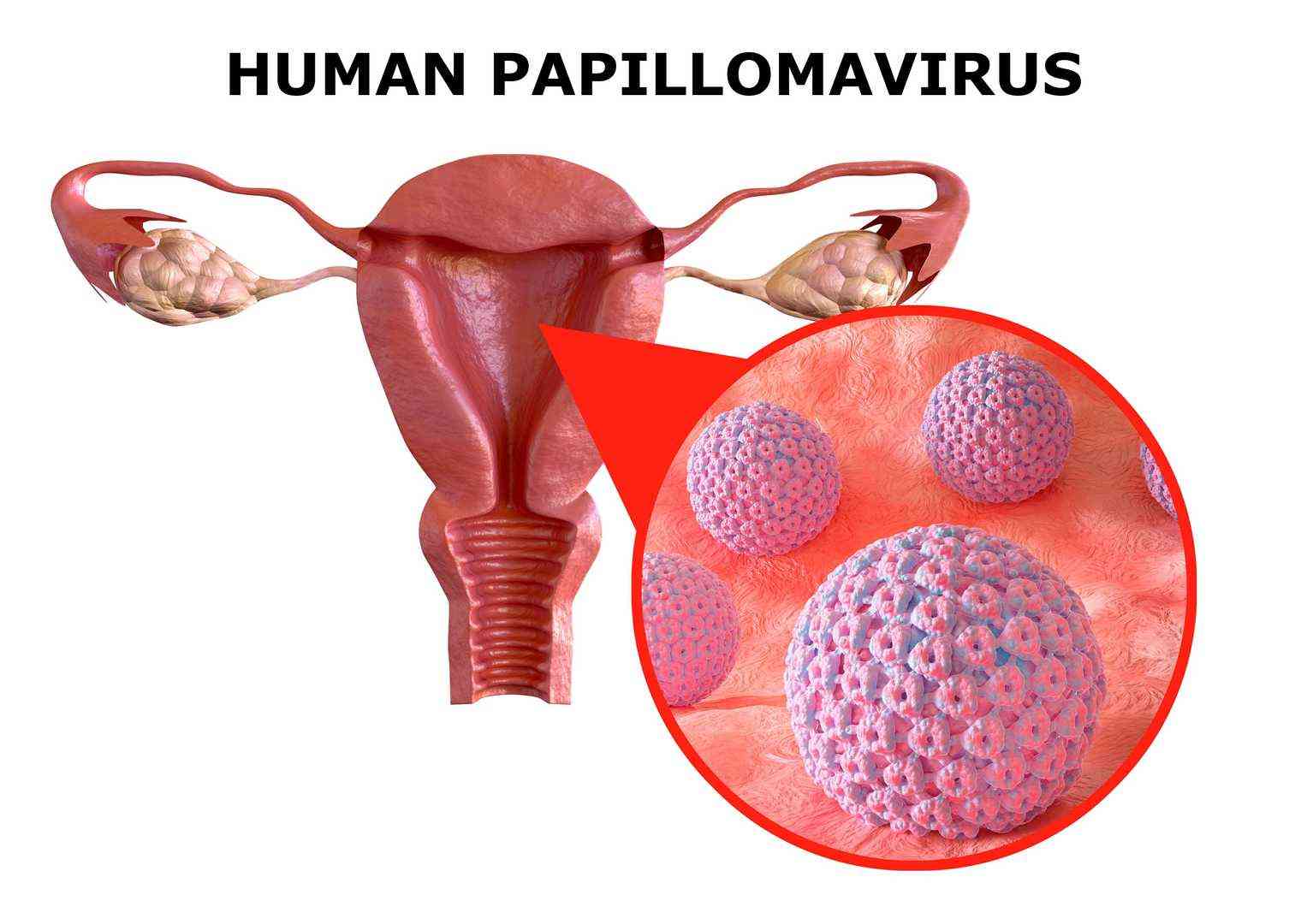
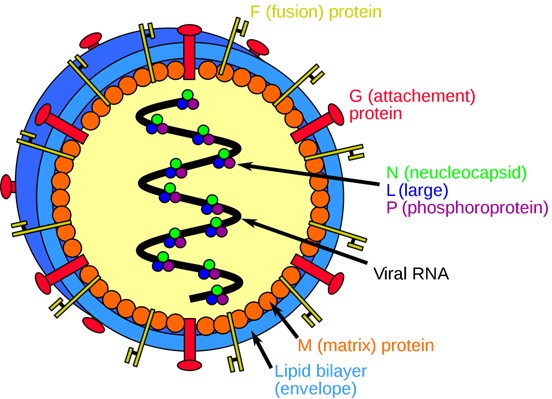 Figure 1. Human Papillomavirus1.
Figure 1. Human Papillomavirus1.
At present, more than 150 subtypes of human papillomavirus have been isolated and identified. According to their pathogenicity or carcinogenic risk, human papillomavirus can be divided into low-risk and high-risk types. Furthermore, based on the different tissue sites invaded, it can be further divided into the following four types:
| Types of Human Papillomavirus | Details |
| Low risk skin type | Related to common warts, flat warts, plantar warts, etc., including human papillomavirus types 1, 2, 3, 4, 7, 10, 12, 15, etc. |
| High risk skin type | It is related to verrucous epidermal dysplasia. Others may include vulvar cancer, penis cancer, anal cancer, prostate cancer, bladder cancer cancer, etc., including human papillomavirus 5, 8, 14, 17, 20, 36, 38. |
| Mucosal low-risk type | Mainly infects the genital, anal, oropharyngeal, and esophageal mucosa, including human papillomavirus types 6, 11, 13, 32, 34, 40, 42, 43, 44, 53, 54, etc. |
| Mucosal high-risk type | Mainly causes cervical cancer, rectal cancer, oral cancer, tonsillar cancer, etc., including human papillomavirus types 16, 18, 30, 31, 33, 35, 39. |
HPV completes initial adsorption by recognizing heparan sulfate proteoglycans (HSPG) on the surface of host epithelial cells, and then binds to integrin α6β4 to trigger endocytosis into the cells. In the late stage of infection, the genome of high-risk HPV types (such as HPV16 and HPV18) can integrate into the host chromosome, and their integration sites are often enriched in the oncogene region (such as MYC locus) or near tumor suppressor genes, laying the foundation for subsequent activation of oncogenic signals.
Core target of E6 protein
Directly binding to the tumor suppressor protein p53, recruiting ubiquitin ligase E6-AP to mediate p53 degradation, inhibiting cell apoptosis and DNA damage repair
Activate telomerase reverse transcriptase (hTERT) to maintain cellular immortality
Combining PDZ domain proteins (such as Dlg1, Scrib) to disrupt cell polarity and adhesion function.
Core targets of E7 protein
Binding to retinoblastoma protein (pRb) and phosphorylating it for degradation, releasing E2F transcription factor to drive cells from G1 phase to S phase
Targeting cyclin dependent kinase inhibitors such as p21 and p27 to relieve their inhibition of the cell cycle
Interacts with histone deacetylase (HDAC) to regulate oncogene expression.
Human papillomavirus (HPV) is widely present in nature and was discovered by German scholar Harald zur Hausen et al. in 1977 in specimens from cervical cancer patients. So far, more than 150 types have been identified. HPV virus can be detected in 90% of cervical cancer and 50%~75% of penile cancer tissues, and is mainly infected with HPV16 virus. Cervical cancer is the second leading cause of death among women with cancer, with 300000 deaths worldwide each year. In recent years, research has also found that about 20% of patients with head and neck squamous cell carcinoma, such as laryngeal cancer, nasal cancer, and nasopharyngeal cancer, can have HPV16 virus detected in their tumor tissues. DNA humans are the only hosts of human papillomavirus, and human infection with HPV is very common with a high infection rate. Generally, cervical HPV infection is age-related, with a peak age of 15-25 years old, which is the main cause of cervical cancer.
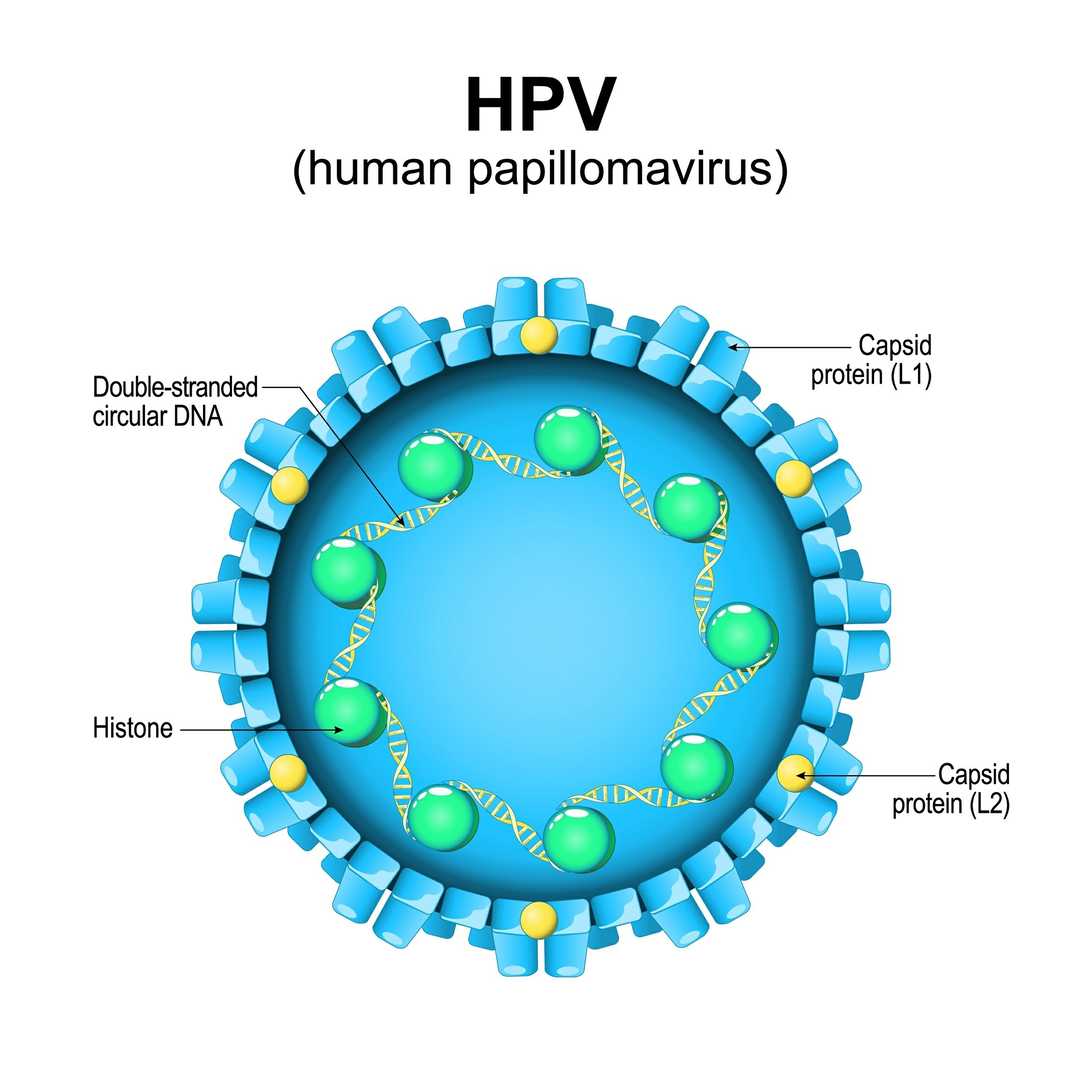 Figure 2. Structure of Human Papillomavirus.
Figure 2. Structure of Human Papillomavirus.
The transmission routes of human papillomavirus mainly include contact transmission, sexual transmission, and mother to child transmission, as follows:
After being infected with human papillomavirus, treatment is required, which can include physical therapy, drug therapy, immunotherapy, and surgical treatment.
| Types of Human Papillomavirus | Details |
| Physical Therapy | Including microwave, laser, electrocautery, cryotherapy, photodynamic therapy, etc., can remove visible tumors and subclinical infections. |
| Drug Therapy | Mainly using 5% imiquimod, 50% trichloroacetic acid, 0.5% podophyllotoxin tincture, fluorouracil ointment, etc., can solve the problem of local skin lesions. |
| Immunotherapy | The purpose is to reduce recurrence and accelerate lesion clearance, and drugs such as isotretinoin, interleukin, interferon, thymosin, BCG, and transfer factor are often selected. |
| Surgical Treatment | In addition to targeting pathogen infections, surgical treatment can be performed for large-scale lesions. For cervical cancer patients, surgical treatment can be performed according to the situation, supplemented by radiotherapy and chemotherapy. |
In addition to vaccination, the best way to prevent human papillomavirus infection is to avoid direct contact with infected individuals, and also to avoid contact with daily necessities, clothing, etc. used by infected individuals. Due to the fact that human papillomavirus is an important pathogen of sexually transmitted diseases, emphasizing sexual safety education and social management can help reduce infections.
Reference
| Target | Cat. No. | Product Name | Host | Isotype | Application | |
| HPV L1 | DMAB-CS23001 | Mouse Anti-HPV L1 Monoclonal antibody, clone 55F10 | Mouse | IgG | ELISA | Inquiry |
| DMAB-CS23002 | Mouse Anti-HPV L1 Monoclonal antibody, clone 56B5 | Mouse | IgG | ELISA | Inquiry | |
| DMAB-CS23003 | Mouse Anti-HPV L1 Monoclonal antibody, clone 56G9 | Mouse | IgG | ELISA | Inquiry | |
| DMAB-CS23004 | Mouse Anti-HPV L1 Monoclonal antibody, clone 58E3 | Mouse | IgG | ELISA | Inquiry | |
| DMAB-CS23005 | Mouse Anti-HPV L1 Monoclonal antibody, clone 15F9 | Mouse | IgG | ELISA | Inquiry |