The abnormal immune attack on self-tissues defines autoimmune diseases which represent a significant worldwide health burden. These diseases usually persist over time while showing frequent relapses and causing intense inflammation. Therapies that include corticosteroids and immunosuppressants typically show restricted effectiveness or result in severe side effects. Pyrrolobenzodiazepines (PBDs) represent a novel category of compounds with distinctive chemical structures and multiple pharmacological effects which show great potential to transform the treatment of autoimmune diseases.
PBDs represent heterocyclic molecules that combine a fused pyrrole ring with a benzodiazepine core into a rigid five-membered structure. The structural framework enables multiple functional adjustments through groups like hydroxyl, amino, or methoxy which precisely control the biological activity. Researchers produce unique compounds like Anthramycin (C12H17Cl2N3) and Chicamycin (C21H25N5O2) through molecular variations which demonstrate distinct pharmacological properties. PBDs cause cytotoxic effects because they form covalent connections with DNA inside the minor groove. In oncological applications this mechanism functions as a crucial component while also enabling immunomodulation by targeting hyperactive immune cells.
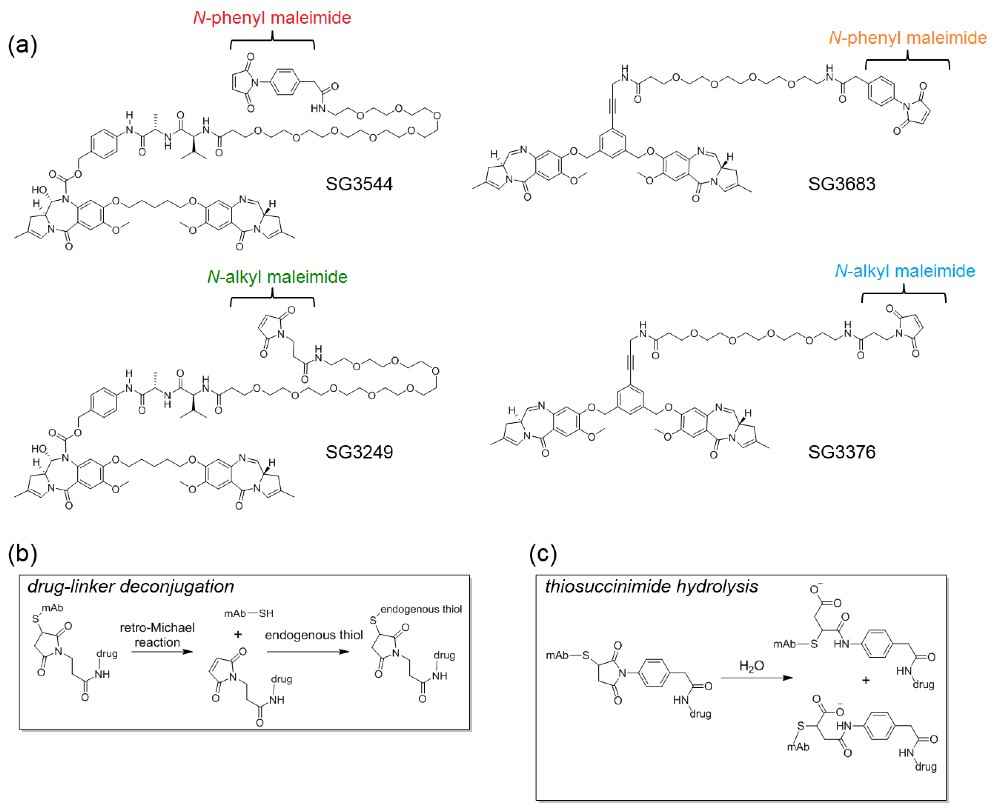 Figure 1. Chemical structures of pyrrolobenzodiazepine (PBD) drug linkers. (Sources: Christie RJ, et al. 2017)
Figure 1. Chemical structures of pyrrolobenzodiazepine (PBD) drug linkers. (Sources: Christie RJ, et al. 2017)
PBDs influence immune pathways through multiple mechanisms, making them attractive for autoimmune therapy:
Midazolam and similar PBDs prevent tissue damage in RA and SLE by inhibiting pro-inflammatory cytokines including IL-6 and TNF-α. The compounds can lessen chronic inflammation through reducing cytokine storms without causing general immune suppression.
PBDs bind to central benzodiazepine receptors which results in neurotransmitter modulation and subsequently decreases both T-cell growth and B-cell antibody production. Dual action therapy targets the fundamental disease mechanism of AIDs through autoreactive lymphocytes that attack the body's own antigens.
PBD dimers in antibody-drug conjugates like Tesirine (SG3249) trigger apoptosis in cells that divide quickly. Originally developed to treat cancer this method holds potential for removal of harmful immune cells in challenging autoimmune disorders.
The antibacterial mechanism of certain PBDs like Anthramycin involves interference with bacterial efflux pumps. This dual function capability connects infections to autoimmune flare-ups and helps decrease disease-triggering factors.
The limited availability of direct clinical trials on PBDs for autoimmune diseases does not overshadow the extensive preclinical evidence proving their versatility. Pyrrolo[3,2-d]pyrimidine derivatives show anti-autoimmune properties in cell culture models by inhibiting the inflammatory pathways related to SLE and psoriasis. The pyrlopyrimidine-based BTK inhibitor Ibrutinib demonstrates RA treatment effectiveness through B-cell signaling inhibition which PBD analogs may further enhance by achieving greater specificity.
Notably, PBD-containing ADCs like CS5001 (targeting ROR1) and ADCT-601 (targeting Mipasatinib Uzoptirine) underscore the adaptability of PBD payloads. These constructs provide targeted destruction of hyperactive immune cells while reducing unintended damage to other tissues which represents a key improvement compared to standard immunosuppressant treatments.
Traditional immunosuppressants, such as methotrexate or cyclosporine, often suppress the entire immune system, increasing infection risks. In contrast, PBDs offer a nuanced approach:
However, challenges persist. Clinical oncology trials show that the high potency of PBDs requires precise dosing to prevent systemic toxicity. Optimizing delivery systems (such as nanoparticle carriers or cell-specific antibodies) remains essential to expand therapeutic windows.
The next phase of PBD research should focus on:
1. Disease-Specific Targeting: Engineering PBD conjugates that home to autoimmune-affected tissues (e.g., synovial joints in RA).
2. Combination Therapies: Pairing PBDs with biologics like anti-IL-17 agents to amplify efficacy.
3. Toxicity Mitigation: Developing prodrugs activated only in inflammatory microenvironments.
4. Clinical Translation: Prioritizing trials in severe, treatment-resistant AIDs, leveraging existing safety data from oncology studies.
Pyrrolobenzodiazepines represent a paradigm shift in autoimmune disease therapy. The properties of unique chemistry alongside multimodal immunomodulation capabilities and adaptable drug design methods make them powerful tools in combating complex immune dysregulation. The full potential of ADC technology will be unlocked through its combination with immunology insights despite existing delivery and toxicity challenges. Patients suffering from ineffective treatments now find hope in PBDs which deliver therapies that provide precise effectiveness which leads to a new sophisticated era in autoimmune disease management.
PBDs exert immunomodulatory effects through multiple mechanisms. These compounds utilize their exclusive DNA-binding function to create covalent crosslinks with DNA's minor groove which leads to selective apoptosis in hyperactive immune cells including autoreactive T and B cells. Targeted cytotoxic effects demonstrate potential for treating autoimmune diseases such as lupus and rheumatoid arthritis because pathogenic cells cause tissue damage in these conditions. For instance, midazolam derivatives downregulate CD80 on macrophages, disrupting antigen presentation. Additionally, certain PBDs exhibit antimicrobial properties, potentially mitigating infections that trigger autoimmune flares. This multimodal action-combining precision cell elimination, anti-inflammatory activity, and infection control-positions PBDs as versatile candidates for complex autoimmune pathologies.
The potential of PBDs from preclinical and translational research is evident but direct clinical trials for autoimmune diseases remain scarce. Disruption of JAK-STAT signaling by pyrrolo[3,2-d]pyrimidine analogs produces anti-inflammatory effects in cell models of lupus and psoriasis. The cancer-targeting ADC Tesirine (SG3249) illustrates the ability of PBD payloads to precisely attack and eliminate active immune cells. Research shows that PBD-based ADCs demonstrated an efficacy 100 to 1,000 times superior to current chemotherapy drugs which suggests they can offer similar therapeutic results in autoimmune diseases that do not respond to treatment. Ibrutinib achieves pyrrolopyrimidine-based effectiveness against rheumatoid arthritis by targeting Bruton's tyrosine kinase (BTK) and demonstrates potential based on PBD-like scaffold architecture. Although safety profile optimization continues to present persistent challenges preliminary results indicate that clinical development should move forward more rapidly.
Traditional immunosuppressants, such as methotrexate or TNF inhibitors, broadly suppress immune activity, increasing infection risks and leaving many patients with partial responses. PBDs offer distinct advantages:
Precision: Unlike systemic immunosuppressants, PBD-containing ADCs target specific cell populations (e.g., CD19+ B cells in lupus), sparing healthy immunity.
Multimodal Action: They simultaneously dampen inflammation, kill pathogenic cells, and address comorbid infections.
Potency: ADCs containing PBD dimers demonstrate exponential increases in cytotoxicity compared to traditional drugs which results in lower necessary doses and minimized off-target effects.
PBDs face difficulties from dose-limiting toxicity which is common in oncology studies and require sophisticated delivery systems such as tissue-specific antibodies. Achieving superior results requires maintaining an essential balance between effectiveness and safety which current therapies lack.
Key challenges include:
Toxicity Management: PBDs' DNA-crosslinking activity, while potent, can damage non-target cells. Strategies like prodrug activation in inflammatory microenvironments or improved ADC targeting are under study.
Delivery Optimization: Ensuring PBDs reach autoimmune-affected tissues (e.g., synovium in arthritis) requires novel carriers, such as nanoparticles or engineered antibodies.
Clinical Translation: Limited autoimmune-specific trials exist. Repurposing oncology ADCs (e.g., ROR1-targeting CS5001) could accelerate progress, but regulatory frameworks for repurposed drugs remain complex.
Cost and Accessibility: ADC therapies are expensive; scaling production and reducing costs will be vital for widespread use.
The next decade may see breakthroughs in:
Disease-Specific ADCs: Creating PBD conjugates to target autoimmune biomarkers like anti-dsDNA antibodies in lupus demonstrates a focused drug design methodology.
Smart Prodrugs: Scientists can produce PBD derivatives which activate specifically in inflamed tissues through the use of pH-sensitive or enzyme-cleavable linkers.
Combination Regimens: Using PBDs together with checkpoint inhibitors such as anti-PD-1 helps to establish new immune tolerance standards.
Gene Editing Synergy: The application of PBDs in CRISPR-based treatments achieves selective removal of autoreactive lymphocytes.
References
| Target | Cat. No. | Product Name | Host | Application | |
| PBD SG3199 | CABT-L3117 | Mouse Anti-PBD SG3199 monoclonal antibody, clone 8I7I0B7 | Mouse | ELISA | Inquiry |
| PBD SG3199 | CABT-L3116 | Rabbit Anti-PBD SG3199 polyclonal antibody | Rabbit | ELISA | Inquiry |
| Target | Cat. No. | Product Name | Type | Host | Conjugate | Application | |
| PBD | DAG-WT677K | MC-Val-Ala-PBD [KLH] | Synthetic | N/A | KLH | N/A | Inquiry |
| PBD | DAG-WT677B | MC-Val-Ala-PBD [BSA] | Synthetic | N/A | BSA | N/A | Inquiry |
| PBD | DAG-WZ1008 | PBD SG3199[BSA] | Synthetic | BSA | ELISA, LFIA | Inquiry |
