
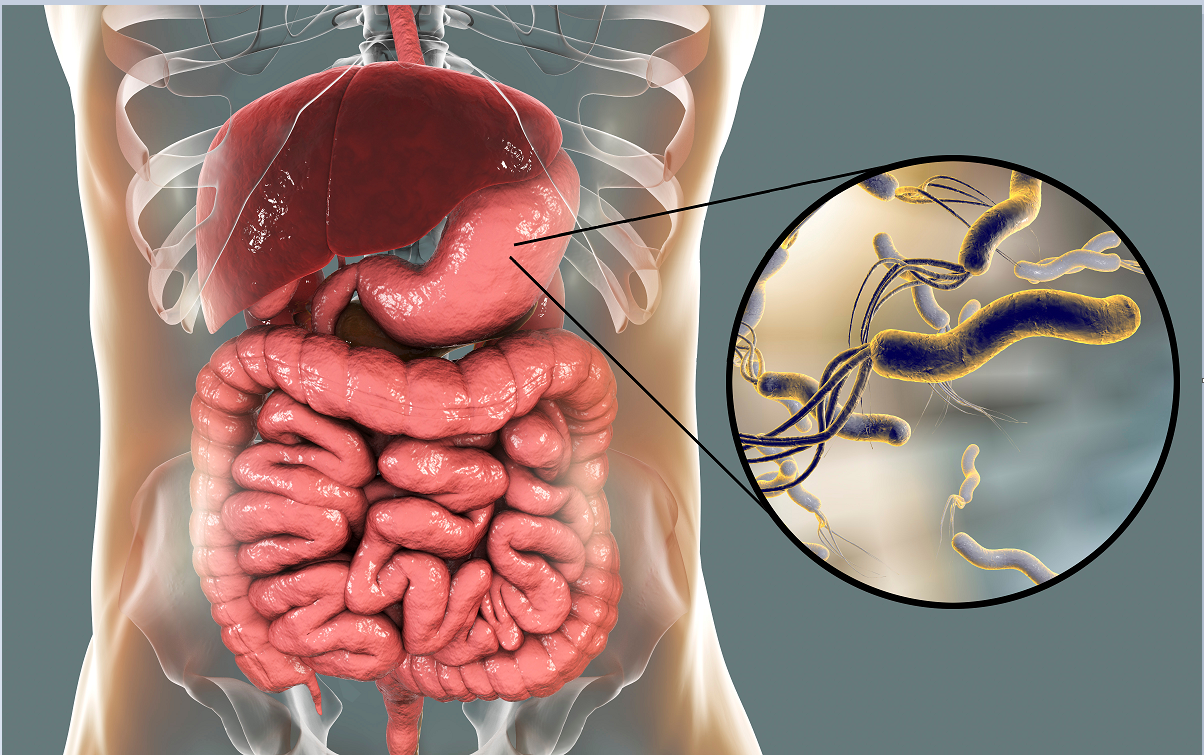
Helicobacter pylori (Hp) spread from East Africa about 58,000 years ago and then developed into different pathogenic strains. Relevant studies have shown that 80% of gastric ulcers and 90% of duodenal ulcers are related to Hp infection. Hp is found in people of all ages in the world, and its prevalence is 20% to 80%. Generally speaking, the prevalence of Hp infection varies with age, region, race, and socioeconomic status. The infection rate of this bacteria is 50.8% in developing countries and 34.7% in developed countries. Due to the huge base of the global infected population and the large number of Hp infections, the accurate, fast and convenient detection of Hp infection is of great significance to the health of the general public. Hp has a set of complete and diverse testing methods, and the choice of testing protocol will depend on the clinical condition, clinician’s experience, testing purpose, cost, sensitivity and specificity. This article reviews the non-invasive detection methods of Hp infection.
Urea Breath Test UBT
UBT uses the urease activity of Hp to decompose urea into ammonia and carbon dioxide. The subjects took the labeled 13C or 14C urea capsules, and the exhaled 13CO2 or 14CO2 was measured by a high-sensitivity specific instrument to determine whether there was Hp infection. Because the 13C-UBT test is not radioactive, it is more suitable for children and pregnant women, but in fact the 14C-UBT radiation dose is very small. In most studies, the sensitivity and specificity of 14C-UBT are more than 90%. UBT is easy to operate, has low technical requirements for inspectors, and has good compliance by inspected personnel, so it is popularized and used in clinical work. UBT has been in use for approximately 30 years and is still the most popular, accurate and universal non-invasive test for diagnosing Helicobacter pylori infection.
15N-urinary Ammonia Excretion Test
The principle is the same as that of UBT. After subjects take orally 15N-labeled urea, it is decomposed by urease, and then the labeled 15NH3 is absorbed by the small intestine and then excreted in the urine. Urine was collected 2 hours after taking the medicine, and the excretion rate of 15N-ammonia in the urine was detected by mass spectrometry to determine the degree of Hp infection in the stomach. This method also has the advantages of convenience, non-invasiveness and less pain for subjects, and compared with 14C-UBT, 15N excretion test is non-radioactive. However, specimen collection, storage and transportation are important reasons that affect its accuracy. In addition, because 15N-ammonia needs to be metabolized in the liver and excreted by the kidneys, there are certain contraindications for patients with liver and kidney insufficiency and false negative results are prone to occur. Some studies believe that probiotics have a certain ammonia-lowering effect, so false negative results may occur. Researchers have shown that the 15N excretion test has a specificity of 81% and a sensitivity of 89%. Because its accuracy is lower than that of UBT, it is rarely used clinically.
Stool Antigen Test Hp-SAT
Hp colonizes on the epithelial surface of the gastric antrum mucosa. As the epithelium of the gastric mucosa is renewed every 3 days, Hp metabolites and dead bacteria are excreted in the feces as specific antigens. Stool antigen detection mainly uses enzyme immunoassay (EIA) and immunochromatography (ICA) to detect related antigens. A retrospective study reported the specificity (93%), sensitivity (91%), positive predictive value (92%) and negative predictive value (93%) of SAT, and it was considered that the coincidence rate of HpSAT with serological examination or UBT exceeded 90%. Some scholars believe that HpSAT based on enzyme immunoassay is more reliable and accurate than the test results based on immunochromatography. Compared with other Hp detection methods, SAT does not require subjects to take any reagents orally and collect test specimens for a long time. The operation is simple and suitable for any age. For subjects with poor compliance or unable to cooperate with the test, SAT is the most beneficial test method.
Serological Testing
Studies have tested Hp’s IgA, IgG and IgM antibodies, but only the IgG antibody test is reliable. Scientists have pointed out that the sensitivity, specificity, and accuracy of the rapid colloidal gold method for detecting Hp are 94.1%, 88.9%, and 93.3%, respectively, and there is no statistically significant difference compared with the 13C breath test. There are also certain differences in the application of different serological testing methods. Through research, scientists believe that the rapid colloidal gold detection method has a higher correlation with the current Hp infection than the western blot method, and is suitable for the preliminary screening of Hp infection; while the western blot method can be used for virulence typing, which is more suitable For the choice of clinical drug treatment. Studies have shown that specific antibodies will only appear in the blood several weeks after the human body is infected with Hp, and the antibodies in the serum can be maintained for more than 6 months after the eradication of Hp. Therefore, a positive serological antibody cannot be used as a basis for current infection, and a negative antibody cannot be used as a non-infection. Because of the possibility of infection, the false negative result of early antibody did not reach the detection threshold. Therefore, when choosing a serological antibody test as a clinical diagnosis result, it is recommended to make a diagnosis in conjunction with UBT. Because of this, researchers proposed that SAT is the only Hp test that is not affected by PPIs, bismuth, antibiotics, and gastric bleeding. If the above-mentioned drug treatment cannot be stopped, SAT is considered to be one of the useful detection methods.